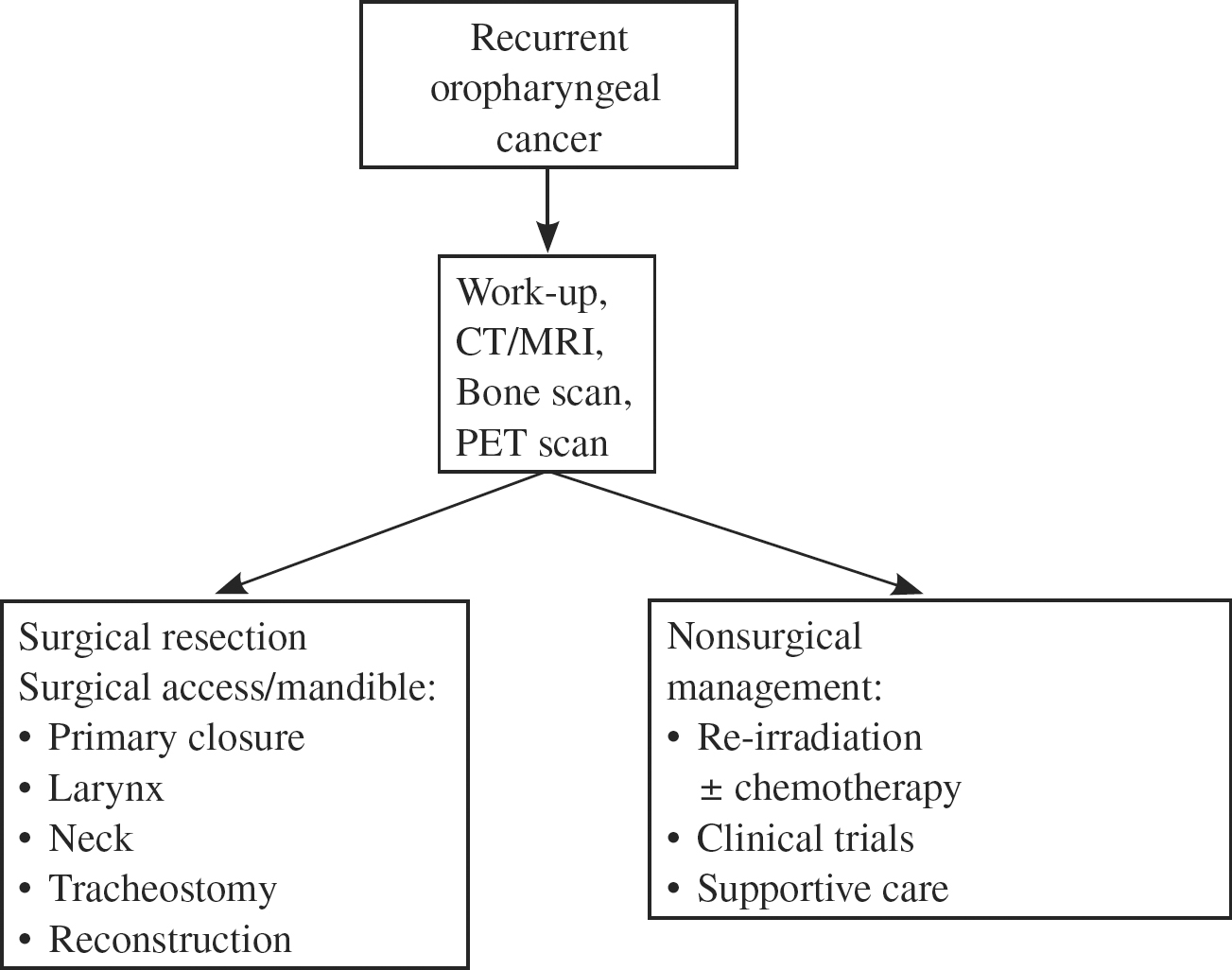
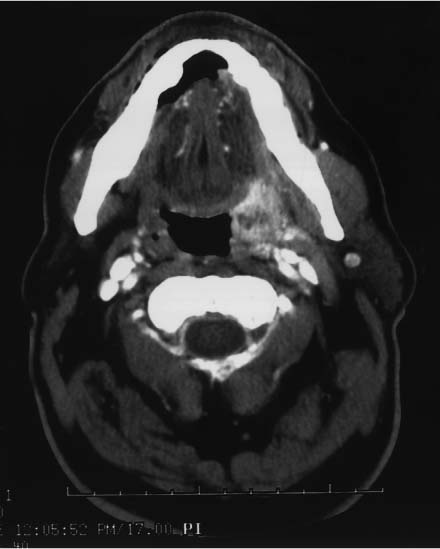
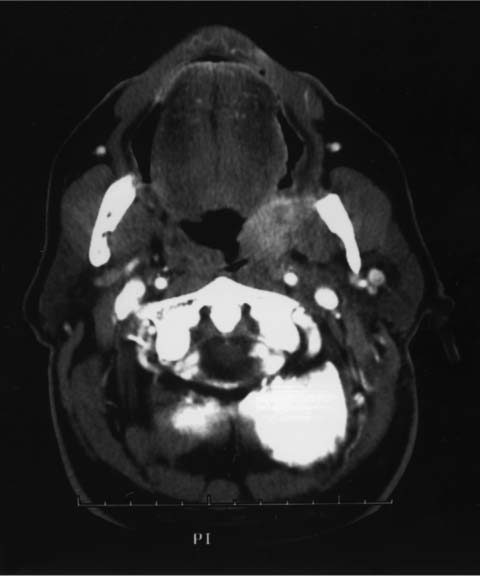
18 Revision Surgery for Oropharyngeal Cancer In 2006, 8950 cases of pharyngeal carcinoma were expected to occur in the United States.1 Approximately one half of oropharyngeal malignancies occur in the base of the tongue, one fourth in the tonsil, and the remainder in the soft palate or posterior pharyngeal wall. Definitive treatment consists of either surgery or radiation therapy for early-stage disease. Later-stage disease usually requires combination therapy, typically using radiation and concomitant chemotherapy or in selected cases surgery followed by radiation and chemotherapy for adverse pathologic findings. The role of combinations of chemotherapy and radiation therapy for stage III and IV disease has come about in an effort to improve the quality of life without compromising survival. Unfortunately, local and regional failure continues to be a major determinant of morbidity and mortality. Local and locoregional failure following initial therapy occurs in 11 to 58% of cases, depending on the stage at presentation.2,3 This is true for all primary treatment modalities. Recurrent or persistent disease following aggressive initial treatment presents a challenge to the head and neck surgeon. This chapter will concentrate on the evaluation of the patient with recurrent or persistent malignancy of the oropharynx following initial surgical or nonsurgical therapy. In the untreated patient, the chief goal is to provide an individualized treatment to maximize survival and minimize functional loss. The evaluation for salvage surgery is the same, but the options are more limited. The goal of the chemoradiotherapy approach is to eradicate disease and preserve the primary site function. Therefore, in the initial assessment of this patient, a decision was made that the anticipated functional deficit from an operation would be greater than with radiation. Salvage surgery is likely to result in the same or greater morbidity than the initial operation. Typically, the resection is bigger and the need for reconstruction greater. A realistic evaluation of the chances for local and regional control and a sense of the functional deficit resulting must be accomplished. Only then can one know how to do the operation, when to do the operation, whether to do the operation, and whether there is a realistic expectation to achieve palliation or cure. It is important that the patient and the physician understand and agree upon the goals of therapy. A multidisciplinary approach involving head and neck surgical oncology, radiation oncology, plastic surgery, dental oncology, medical oncology, and others is important to address all aspects of treatment. Decisions must be made on a continual basis and start with the initial decision of whether the therapy is intended to be curative or palliative. Local and regional failure of head and neck cancer has consistently been shown to be one of the most devastating afflictions due to the high degree of pain, functional loss, disfigurement, and reduction in quality of life. Therefore, either cure or palliation can be reasonable goals of surgical therapy. Pain relief may be better achieved by surgical therapy.4 The presence of distant metastases does not necessarily exclude surgery as a treatment modality if an operation can be done with a reasonable expectation of recovery, a diminution in the likelihood for pain and uncontrolled local growth, and a life expectancy that is long enough to make the short-term recovery from surgery worth the longer-term benefit. This is typically at least 6 months. Although recurrent laryngeal cancer frequently meets these criteria, oropharyngeal cancer surgery, due to the cancer’s lack of clear anatomical barriers and the morbidity associated with the operation, is less likely to be an option for palliative treatment. Thus, a more extensive evaluation for distant metastases should be done prior to salvage surgery to get an estimate of survival. A more extensive work-up individualized to the patient may include a chest and abdomen computed tomography (CT) scan, bone scan, or positron emission tomography (PET) scan. Similarly, patients who have persistent disease after treatment or who recur within 6 months after the completion of treatment tend to have a much worse prognosis and limited life expectancy and are less likely to be candidates for salvage surgery. The surgeon must weigh the surgical options and likely sequelae against the alternatives. Consideration of the following issues will be important in determining operability and the extent of resection, which will best define the likely sequelae from the operation and be very important in predicting intermediate and long-term quality of life. Each case is carefully individualized and depends on factors related to the patient, the tumor, and what options are available to the treating physician. Decision tree for recurrent oropharyngeal cancer Physical examination coupled with CT and/or magnetic resonance imaging (MRI) is necessary to define the extent of disease and aid in determining operability. Disease that persists or recurs following radiation and chemotherapy is harder to assess clinically due to the fibrosis that accompanies such treatment. The role of PET scanning is currently being defined. At present, it appears that PET may yield important information with respect to the neck but is less accurate in predicting primary recurrence in the oropharynx.5 Ultimately, clinical judgment and biopsies obtained during an exam under anesthesia may be the best way of outlining the extent of recurrence. Even more than with untreated disease, margins are often deceptive, with clinically normal-appearing tissue often harboring infiltrative carcinoma. Frozen section is vital to achieve clearance of disease. Subclinical disease found at frozen section often makes the extent of resection larger than anticipated. This possibility should be taken into account when planning reconstruction so that several options are available. Bone invasion following radiation therapy is more likely and proceeds along less predictable routes than in the untreated setting (Fig. 18.1).6 Bone margins need to be more generous in the postirradiation setting. Marginal mandibulectomy may be hazardous in the postirradiation setting due to the unpredictable nature of invasion, the risk of mandibular fracture, and the potential increased risk of osteoradionecrosis. It is important to determine in advance if the carotid artery is likely to be involved by tumor and have a preoperative management strategy mapped out (Fig. 18.2). If one is going to leave tumor on the artery, it is not likely that the operation will result in significant success, and a radical resection of the oropharynx is probably not warranted. If the artery is to be resected, then one should be prepared for reconstruction at the time. This can be very difficult with oropharyngeal cancers because involvement of the carotid is typically high near the skull base. Ligation of the artery without prior balloon occlusion studies imparts a significant risk of neurological injury and thus is probably not a reasonable palliative procedure. Similarly, clearance of disease from the skull base can be assessed preoperatively; if the expectation is low, other options should be considered. Fig. 18.1 Computed tomography scan demonstrating recurrent squamous cell carcinoma following concomitant chemotherapy and radiation. Tumor extends to the mandible without obvious involvement. Pathologically, the tumor extended into the bony cortex.
Patient Evaluation
Determining the Extent of Resection
Assessment of the Mandible
Assessment of the Carotid Artery
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Revision Surgery for Oropharyngeal Cancer
