29 Revision Surgery for Non-melanoma Skin Cancer Non-melanoma skin cancer (NMSC), comprising primarily squamous cell carcinoma (SCC) and basal cell carcinoma (BCC), has emerged as a global health problem of epidemic proportions. Epidemiologic surveys have estimated that 1.3 million cases are diagnosed each year in the United States, with 2.75 million new cases worldwide. Unlike other forms of cancer, the incidence is expected to rise at alarming rates over the next 30 years.1,2 The economic impact of this disease is burgeoning as well, with over $425 million spent per year on the diagnosis and treatment of NMSC within the Medicare population of the United States.3 The recognized association between these lesions and sun exposure dictates that cutaneous SCC and BCC typically arise on sun-exposed areas of the body, with > 80% of the lesions appearing on the head and neck. Despite the frequency with which cutaneous malignancies arise on the head and neck, the majority of lesions are evaluated and treated by our colleagues in dermatology or even primary care. However, more advanced lesions, such as recurrent, deeply invasive, and metastatic lesions, remain the purview of the head and neck surgeon. We will discuss our management of these aggressive skin malignancies, describing our pretreatment assessment, the principles employed in treating the various subsites in the head and neck, and an overview of the current controversies such as indications for parotidectomy, neck dissection, and temporal bone resection. Also, we will describe available adjuvant or alternative therapies, including chemotherapy, radiation, and re-irradiation. Due to the broad scope of cutaneous SCC and BCC, we will limit our description to non-melanoma skin cancer. In our opinion, cutaneous melanoma represents a different biologic entity with unique pathophysiology and behavior whose management merits separate discussion. The majority of cutaneous SCC and BCC cases arise on sun-exposed areas of the body, accounting for the disproportionate incidence of these lesions on the head and neck. Exposure to ultraviolet radiation, particularly ultraviolet B (UVB) light, has been identified as the primary risk factor for developing NMSC. Once present, a typical NMSC may be treated with any number of techniques, including electrodissection and curettage, cryotherapy, simple excision, topical agents, and even radiotherapy. Cure rates from all of these modalities are comparable, ranging from 90 to 98% across numerous studies. The widespread availability of Mohs micrographic surgery, a technique in which horizontal frozen section analysis is performed in an attempt to achieve total margin control, has improved cure rates for NMSC to ~99%.4 Nevertheless, a subset of NMSC exists that defies these accepted modalities and demands more aggressive therapy. Lai and colleagues have described the features of aggressive NMSC, in terms of their propensity to recur, invade, and metastasize.5 Recurrent tumors, lesions > 2 cm in maximum dimension on initial evaluation, and those exhibiting rapid growth or regional metastases are commonly considered aggressive NMSC. Poorly differentiated or spindle cell SCC, as well as morpheaform and basosquamous forms of BCC, constitute more virulent histopathologic variants.5 Finally, lesions located in the central “H zone” of the face or at sites of embryonic fusion planes, such as the glabella, nasal root, and melolabial sulcus, have been noted to exhibit more aggressive behavior, with deep invasion occurring prior to extensive surface expansion.6,7 Lesions that fit many of these characteristics are more likely to recur following initial treatment, and these are the lesions with which the head and neck surgeon will be faced. With recurrence also comes the issue of advanced disease, metastases, and invasion into adjacent structures, such as the orbit and temporal bone. Thorough patient evaluation and critical decision making with regard to parotidectomy, neck dissection, temporal bone resection, and the use of adjuvant therapies will maximize the ultimate result in terms of local and regional disease control and survival. Patients with recurrent NMSC who present to a head and neck surgeon have usually been referred by a dermatologist, plastic surgeon, otolaryngologist, or other practitioner. Nevertheless, as with all conditions, a thorough history and physical examination are the cornerstone of patient evaluation, although radiographic images provide invaluable data for treatment planning. The risk factors for NMSC are widely known and are summarized in Table 29.1. Key features in the history include the extent and severity of previous sun exposure, exposure to ionizing radiation, and immunosuppression from infectious, neoplastic, or iatrogenic causes, as in the case of organ transplant patients. Patients should be queried about the duration of the lesion in question, the rapidity with which it has grown, the presence of subjective facial weakness or asymmetry, and the detection of any locoregional pain or paresthesias. Table 29.1 Risk Factors for Non-melanoma Skin Cancer
Aggressive Non-melanoma Skin Cancer
Patient Evaluation
Historical Points
Ultraviolet Radiation B Exposure |
Patient Characteristics |
– Light skin color |
– Inability to tan, easily burns |
– Light eye color |
Precursor Lesions |
– Bowen disease |
– Actinic keratoses |
Immunosuppression |
Syndromes |
– Xeroderma pigmentosum |
– Nevoid basal cell syndrome |
– Albinism |
– Epidermodysplastic verruciformis |
– Epidermolysis bullosa dystrophica |
Ionizing Radiation |
Polycyclic aromatic hydrocarbons |
A detailed dermatologic history is mandatory, focusing on the location and previous management of all prior lesions on the head and neck, including premalignant conditions such as actinic keratoses. If possible, medical records, operative notes, and pathology reports should be reviewed for previous treatment of the lesion (s) in question. The pathology reports in particular provide key information regarding the status of surgical margins, depth of invasion, and the presence of perineural invasion—this information may be augmented by having the dermatopathologist review the actual slides or tissue blocks from the outside facility.
Physical Examination
In addition to performing a complete head and neck examination, attention should be focused on the lesion of concern, its relationships to surrounding structures, and the lymph node basins that provide first and second echelon drainage for the anatomical subsite of the head and neck. Careful assessment of the lesion and its mobility relative to adjacent structures is important. Nonmelanoma skin malignancies may directly invade the cartilage of the external auditory canal and the bone of the craniofacial skeleton, including the mandible, midface, orbital rim, and calvarium. Preservation of the skin’s innate mobility over the underlying bony and cartilaginous framework suggests that these structures are not involved. The external auditory canals and tympanic membranes merit scrutiny under the operating microscope in the setting of an auricular or preauricular primary, as sleeve resection of the external auditory canal and lateral temporal bone resection may be determined based on the visible invasion of the lesion toward or into the middle ear. For periorbital lesions, the eye should be assessed for proptosis, chemosis, extraocular mobility, and visual acuity, as any impairment of ocular appearance or function may suggest gross invasion into the orbital cavity or perineural spread along the infraorbital nerve (V2) or the supraorbital and supratrochlear nerves (V1).
Palpation of the neck, including the parotid gland, may determine whether a parotidectomy or neck dissection will be undertaken. Lymph node metastases in NMSC are more common in SCC, occurring with an incidence of 0.5 to 16%.8 BCC metastases do occur, but the incidence is negligible. The nodal basins most commonly involved by NMSC depend on the location of the primary lesion, as depicted in Fig. 29.1. Lesions of the ear, lateral cheek, and periorbital and temporal regions commonly drain to lymph nodes within the parotid gland, whereas occipital, upper jugular, perifacial, and submandibular lymph nodes provide common avenues for most other sites in the head and neck. When the parotid gland is involved by metastatic NMSC, up to 26% of patients will have clinical involvement of the cervical lymphatics, with ~33% of patients with clinically negative necks exhibiting pathologic nodal involvement.9 The lymphatics accompanying the external jugular vein are also important sites of metastasis in NMSC. The cervical lymphatics on the contralateral side should also be examined, as lesions of the midface and lip exhibit a propensity for bilateral metastases.
Cranial nerves must also be examined, with particular emphasis on the branches of CN V and VII that innervate the area of the primary lesion, as these nerves are commonly involved by perineural tumor spread.10 Perineural tumor invasion represents a form of direct tumor extension, rather than a metastatic focus of disease. Aberrant sensation or subtle facial weakness may be detected on close evaluation, although these are commonly late findings.
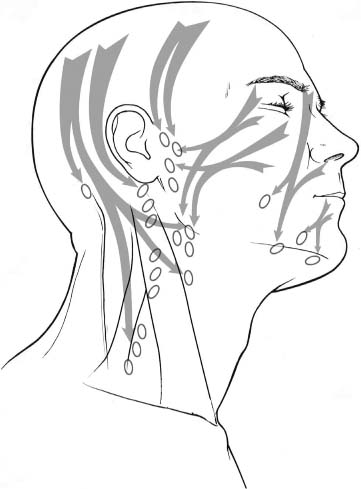
Fig. 29.1 Lymphatic drainage pathways of the skin of the head and neck. Lymph nodes within the parotid bed, the perifacial nodes, and those in levels II and III provide the most common avenues for lymphatic metastases. Anterior lesions involving the lip and midface may exhibit bilateral drainage. Lymph nodes along the external jugular vein also provide a common avenue for metastasis. Note that posterior scalp lesions may spread directly to level V along the spinal course of accessory nerve.
Imaging
We regard imaging as imperative in the preoperative assessment of the aggressive NMSC patient. Although physical examination can provide important information regarding the location of the lesion, its fixation to underlying structures, and motor or sensory nerve malfunction, imaging provides the key data that determine the operative plan. Computed tomography (CT) scanning is the most common modality employed, as it details the extent of soft tissue involvement, bony destruction, spread into the middle ear and temporal bone, orbital extension, and the presence of parotid or cervical lymphatic metastases. By depicting widening of neural foramina or the pterygomaxillary fissure, it can reveal subclinical perineural invasion.10
Magnetic resonance imaging (MRI) is used selectively, depending on the location of the lesion and the clinical findings. For deeply invasive scalp lesions, MRI can demonstrate the relationship of the tumor to the dura and vascular structures such as the sagittal sinus. MRI is invaluable in the evaluation of perineural invasion because the affected nerve may be subtly thickened along its proximal course to the skull base. Because deeply invasive lesions may spread to the skull base or sinonasal cavities, MRI is also useful in the differentiation of tumor from secretions. Finally, patients routinely undergo standard chest plain films to screen for pulmonary metastases.
Surgical Management
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


