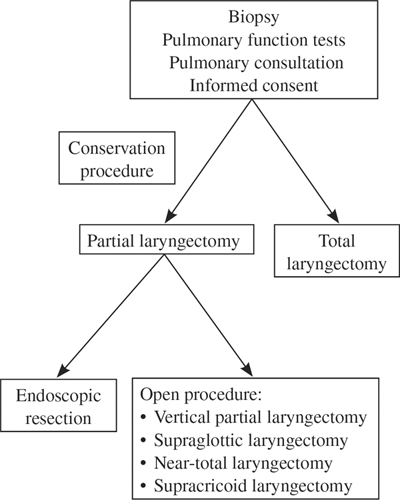
19 Revision Surgery for Early Carcinoma of the Larynx This chapter will explore the indications for and the special problems associated with attempts to surgically salvage a functioning larynx following local failure of primary surgery and/or radiotherapy/chemotherapy for the cure of early carcinoma of the larynx. With the advent of better and more widely available radiotherapy and, in some circumstances, the application of adjuvant chemotherapy, conservation surgery has been employed less frequently in recent years as the primary modality for early or moderately advanced carcinoma of the larynx. Even when conservation (subtotal) laryngeal surgery was used more commonly than it is now, radiotherapy was usually incorporated into planned pre- or postoperative management for all but the earliest malignancies.1 Local persistence of disease is relatively uncommon following planned, combined surgery and radiotherapy for even moderately advanced cancers of the larynx (i.e., most failures are in the neck) and almost unheard of after partial laryngectomy for early glottic lesions. More often, head and neck surgeons are called upon to attempt to salvage larynges with persistent cancers after failed radiotherapy and/or chemotherapy were used in an attempt to achieve a single-modality cure. When it is still possible in such cases, subtotal laryngectomy can be considered a form of revision surgery. Conservation surgery may be defined as resection of tissue adequate to remove all apparent carcinoma with clear margins, while “conserving” enough tissue to permit functional reconstruction. Conservation surgery should not be confused with conservative surgery. This approach is not conservative, because all eventual surgical cure rates for any given lesion must be compared with those that can be achieved with total laryngectomy. When a physician elects to attempt surgical cure by a procedure less extensive than total laryngectomy, the onus is upon him or her to ensure that the lesion does not eventually persist in the laryngeal remnant “conserved” for functional reconstruction. In the larynx, conservation procedures may be classified according to the location of the original lesion and/or the portion of the larynx that must be removed and reconstructed in an attempt to cure it. Generally, these procedures are referred to as (1) vertical partial laryngectomy (hemilaryngectomy), (2) horizontal partial laryngectomy (supraglottic laryngectomy), or (3) near-total laryngectomy. Any of these procedures may be applicable after persistence of carcinoma treated either by radiotherapy or previous partial laryngectomy, provided that the lesion can be removed with clear margins, leaving sufficient tissue to permit eventual functional reconstruction. Certain principles must be observed, and, particularly after failed radiotherapy, special precautions must be taken to increase the likelihood of eradication of tumor as well as successful reconstruction when subtotal laryngectomy procedures are attempted for salvage. In the days when subtotal laryngectomy was often undertaken following planned preoperative radiotherapy, it was understood that the excision of tissue necessary to achieve reliable cure rates was that which would have been appropriate to the extent of the original lesion, before any tumor reduction that might have occurred as a result of radiotherapy.2 Therefore, the decision to attempt conservation salvage surgery following failed radiation/chemotherapy for cure must follow the same principle.3 Moreover, the surgeon must remember that the pathologist’s ability to accurately evaluate frozen section tumor margins may be compromised by previous radiotherapy. This is particularly true within the 3 to 4 months immediately following completion of radiotherapy/chemotherapy, during which period individual cells are often distorted and may mask the criteria needed to evaluate the extent of residual disease. It is possible, however, to safely explore larynges with residual disease with the intent of carrying out a conservation procedure. In the study by Tucker, there was no difference in local tumor control rate among a group of patients with T2 and T3 cancers of the larynx when subjected to initial en bloc total laryngectomy versus attempted partial laryngectomy, some of whom were then converted to total laryngectomy when intra-operative findings indicated that subtotal laryngectomy would have been inadequate.4 Local control was comparable to total laryngectomy, as well, in the subgroup of patients who could be resected successfully by conservation technique. Because many patients with persistent disease following failed radiotherapy/chemotherapy and most of those who have failed initial attempted subtotal laryngectomy will have lesions that are “borderline” for salvage by partial laryngectomy, it is essential that permission for total laryngectomy be obtained in every case. Decision tree for recurrent early larynx cancer Most classic partial laryngectomies are reconstructed with local tissues preserved for that purpose.5 However, this residual tissue must not be “saved” at the expense of tumor resection sufficient to obtain local control. In cases where previous radiation/chemotherapy or partial laryngectomy have failed, residual local tissue that can be preserved after further resection will be, at best, strictly limited and, at worst, inadequate for safe functional reconstruction. Although it is seldom necessary to employ local or regional flaps in reconstruction of primary partial laryngectomy, it is very often necessary when secondary conservation surgery is undertaken. Selection of adjunctive means of secondary reconstruction must depend on the patient’s medical condition and ability to tolerate extended procedures, the surgeon’s experience and capability, and reasonable expectations for survival. For example, electing to use a free flap in such a case adds significant surgical time, morbidity, and expense. If the patient is in poor physical condition or has other, intercurrent disease that is likely to significantly shorten life expectancy, has other risk factors, such as diabetes or peripheral vascular disease, that can impact on the likelihood of successful vascular anastomosis, or if available surgical experience with distant revascularized flaps is limited, a more conservative form of reconstruction should be considered. Although pectoralis major myocutaneous flaps can be useful in reconstructing extended supraglottic laryngectomies, they tend to be more bulky than is either necessary or useful, but they can usually be accomplished as a one-stage procedure.6 Whereas this characteristic of myocutaneous flaps may often be advantageous, in postradiation/chemotherapy failures, it is advisable to reconstruct in two stages, incorporating a planned, dependent fistula in the first stage. Most cases of extended supraglottic laryngectomy that require tissue augmentation can be managed with an undelayed, medially based deltopectoral flap (Bakamjian flap) (Fig. 19.1).7,8
Conservation Laryngectomy
Principles and Precautions
Adequate Tissue Removal
Reconstruction
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Revision Surgery for Early Carcinoma of the Larynx
