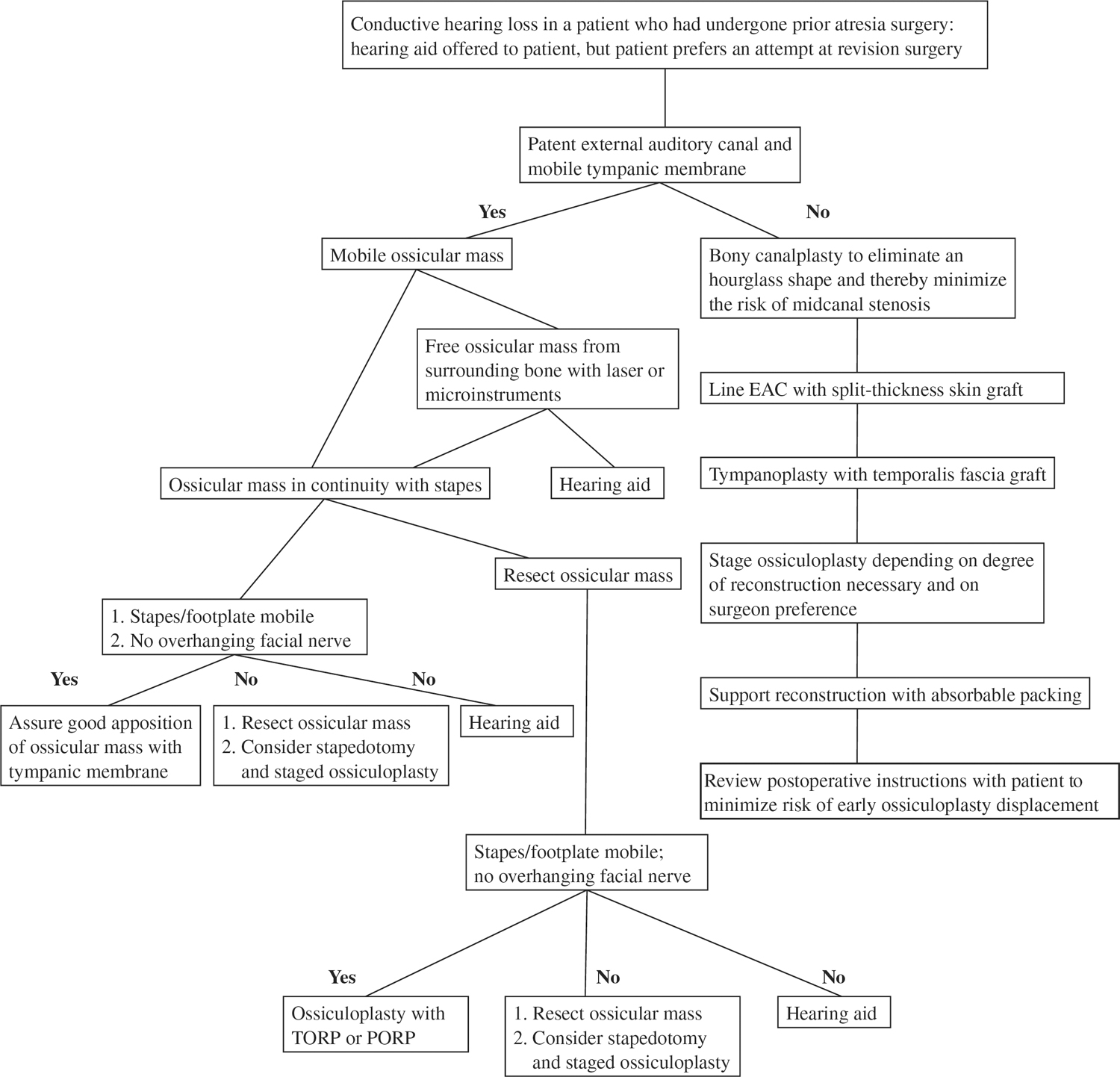
13 Revision Surgery for Congenital Aural Atresia Learned otologists have stated that the surgical repair of congenital aural atresia is among the most difficult tasks in otology. It follows, then, that revision atresia surgery represents an even more daunting task. As is so often true in otologic surgery, the key to success in this enterprise resides in the details. In revision atresia surgery, the pre-operative assessment and planning require great circumspection, and the operative technique must be meticulous. In the common scenario of revising another surgeon’s first repair attempt and in situations where the cause of the previous surgical shortfall is not immediately apparent, the operative repair is best undertaken in a stepwise fashion. Finally, conscientious and thorough care is required in the early postoperative period to optimize the course of healing and to avoid incipient complications. The difficulty of atresia surgery is perhaps best illustrated by the high revision rate that may be anticipated even in the hands of the most experienced otologist. It is expected that up to one third of surgical atresia repairs will require some greater or lesser degree of revision surgery to achieve optimal results in hearing rehabilitation and freedom from infection.1 In various series, revision rates were 34% (17 of 50 primary surgeries),1 30% (21 of 69),2 32% (20 of 63),3 30% (6 of 20),4 and 33% (8 of 24 major atresia repairs).5 Later series involving some of the same primary surgeons demonstrated decreases to 19% (3 of 16 primary repairs)6 and 22% (13 of 58),7 perhaps a reflection of refinements of technique. When discussing revision surgery for congenital aural atresia with the patient, the option of a bone anchored hearing aid must be considered. Indeed, this device must be mentioned at the time of the initial assessment for aural atresia, just as a hearing aid is for otosclerosis. In this chapter, however, the focus will be on surgical management of the ear canal and middle ear. In the initial consideration of surgical revision, the reasons for failure of the primary repair must be determined, if possible. When infection and otorrhea are the primary patient concern, the history will immediately make this apparent. When the principal issue is suboptimal hearing rehabilitation, clinical clues may be valuable in determining the origin of the ongoing conductive hearing loss (CHL). The patient’s failure to achieve marked subjective hearing improvement in the immediate postoperative period (from packing removal to about 2 months postoperatively) is suggestive of an immediately displaced prosthesis or an occult ossicular chain abnormality that was not addressed. The gradual onset of CHL over months or years implicates the healing mechanism in the cause of hearing loss; if the patient also has undergone a columella-type reconstruction using either artificial or autologous materials, the possibility of adhesions causing ossicular chain disarticulation or ankylosis is high. Lateralization of the tympanic membrane graft or thickening due to chronic inflammation is also consistent with this time course and should be evident to the careful microscopic ear exam. One would not expect a severe conductive hearing loss solely from external canal stenosis until the stenosis is very advanced (opening ≤ 2 mm). Although otitis media is not a frequent concern in children with congenital atresia (perhaps due to selection bias against operating on the hypopneumatized middle ear cleft), the possibility of middle ear fluid, which may not be apparent through the reconstructed tympanic membrane, must be considered. Rarely, a patient may note daily hearing fluctuations in the context of barometric or body positional changes, suggesting a partially reversible ossicular chain discontinuity as might occur in repairs employing a stapes piston or a nonbiointegratable artificial prosthesis. In the patient whose chief complaint is residual CHL, the decision to perform revision surgery should be compared with expected hearing results in successful atresia repairs. In the numerous series of atresia repairs, a variety of methods have been used to report hearing results, making comparisons difficult. Nevertheless, review suggests that in candidates for reconstruction, it is reasonable to expect a gain in pure tone average (PTA) of 25 to 30 dB,2,4,6,8 for 40% of patients to achieve a postoperative PTA of ≤ 20dB, and 60% overall to achieve a PTA of ≤ 30dB,2,4,9 with comparable speech reception thresholds (SRTs).6 This translates to a residual air–bone gap of ≤ 20 dB in ~50% of patients and of ≤ 30 dB in 70% of selected patients.3,7,10 Equally interesting to the surgeon considering revision are data concerning the odds of successful hearing rehabilitation in revision repairs. Provided the expectations are appropriately restrained, as in any revision surgery, the prognosis for well-selected patients is quite reasonable. In one revision series of the surgeon’s own primary repairs, 12 of 20 of the patients were able to achieve a < 20 dB residual air–bone gap;3 in another series, four of four revisions obtained a patent external auditory canal (EAC) and achieved “serviceable” hearing (PTA ≤ 40 dB).8 In another series, 53% (8 of 15) of patients undergoing revision attained an SRT of ≤ 30 dB.6 A final factor in decision making is an awareness of the mild progressive CHL that occurs in a large percentage of successful atresia repairs; in such a patient, a revision procedure may be unlikely to yield significant long-term improvement. In a typical series, the natural history of hearing decrement in repairs deemed successful was 19%; this averaged a 20 dB loss over an average 2.6-year follow-up.7 Decision tree for aural atresia revision surgery Individual patient factors are of paramount importance when considering whether to undertake a revision operation for hearing. Numerous surgeons have alluded to subsets of patients with both favorable and unfavorable indicators. For example, in one series an initial very good hearing result was found to be an excellent prognostic sign, whereas the need to use an artificial prosthesis for ossicular chain reconstruction was identified as a significant unfavorable sign.6 As in primary atresia repair, it is prudent to attempt to limit elective surgery to patients with normal or near-normal cochlear function and middle ear anatomy conducive to a repair attempt. Largely through the labors of Jahrsdoerfer and colleagues,11 marked advances have been made in characterizing the anatomical features critical to successful reconstruction of the conductive hearing apparatus. The two most important features appear to be the presence of the stapes and the size of the middle ear cleft. The detection of a stapes on a temporal bone computed tomography (CT) scan simultaneously implies the existence of a patent oval window with a mobile footplate and a facial nerve that does not obstruct the oval window to a degree prohibiting ossicular chain reconstruction. The existence of a middle ear cleft of at least 50% normal area in both coronal and axial CT views6 (compared with age-matched controls or the opposite ear in unilateral atresia) implies that recognizable mesotympanic landmarks exist to guide the surgeon to the otic capsule and the oval window. This “50% criterion” probably further implies that enough mediolateral depth exists in the middle ear cleft to allow reconstruction of the transformer apparatus without subsequent middle ear collapse, a feature long considered critical to lasting hearing rehabilitation in chronic ear surgery. The middle ear cleft is so critical that its absence is an absolute contraindication to a surgical attempt at hearing rehabilitation, whether primary or revision. In the atresia ear requiring reoperation, a knowledge of the frequency of various types of malfunction is informative in both initial and intraoperative assessment. Soft tissue stenosis of the reconstructed external auditory canal (neoEAC) is such a common postoperative problem that one surgeon affirmed that more failures occur due to graft and canal healing problems than ossicular chain problems.10 In accordance with this assertion, many series have cited soft tissue stenosis as the most frequent problem necessitating revision, typically affecting 10 to 25% of patients who have undergone primary repair. In one large series, this rate was 18% (9 of 50 primary repairs),6 in another, 26% (18 of 69).2 Factors important in reducing soft tissue stenosis include the use of split-thickness versus full-thickness skin grafts, meticulous coverage of all exposed bone,10 a generous meatoplasty,12 and the recognition that the more severe grade III microtias have a significantly higher rate of meatal stenosis due to reduced conchal cartilaginous support.6 In a single series, bony restenosis was cited as a complication in 12% of cases (7 of 58 primary surgeries) and a factor in revision in 35% (9 of 26) cases.7 One factor the authors considered important in this adverse occurrence was the youthfulness of their average atresia patient; the presumed higher metabolic bone activity in younger patients predisposed them to “exuberant bone growth.” Nearly as common as the complication of soft tissue stenosis is lateralization of the grafted neo-tympanic membrane (neo-TM). In one large series, this occurred in 8% of cases (4 of 50 primary repairs).6 In another series of 56 primary repairs, lateralization was the most common cause of a poor hearing result, occurring in 14 (25%).3 This complication was noted to ensue most commonly within the first 12 months postoperatively. In a later series from the same group, neo-TM lateralization was a significant factor in 42% (11 of 26) of cases selected for revision.7 It is perhaps noteworthy that this complication occurred in only 9% of primary cases but in 15% of revision cases.7 In another series, TM lateralization requiring revision occurred in only 6% (1 of 16 cases), yet lateralization recurred despite reoperation.6 Such data suggest that either prior surgical trauma or particular anatomical or physiologic patient characteristics may increase the risk of recurrent lateralization during further repair attempts. One anatomical characteristic, the severity of the malleus deformity, has been implicated as a factor in lateralization. Specifically, it has been noted that an absent or rudimentary malleous makes medial fixation of the fascia graft more difficult and less predictable.6 Ossicular chain malfunctions are another significant cause of failure of primary surgical repair. Ossicular fixation is perhaps the most common problem of this type; in one series this rate was 3.4% (2 of 58 primaries).7 Again, it is noteworthy that this rate climbed to nearly 8% in the revision cases in this series, suggesting that, like lateralization, this problem may be exacerbated by particular patient anatomical factors or by operating in previously violated territory. Certainly the patient with a low tegmen would seem to be at higher risk for bony or fibrotic refixation of the lateral ossicular mass to the epitympanum. The anatomical abnormalities common to atresia ears may also predispose to medial ossicular chain fixation. In 11% (8 of 71) of one surgeon’s series, the stapes was found to be small and fixed to the fallopian canal.7
Indications for Revision
Causes of Surgical Failure
Canal Stenosis
Tympanic Membrane Lateralization
Ossicular Chain Malfunction
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Revision Surgery for Congenital Aural Atresia
