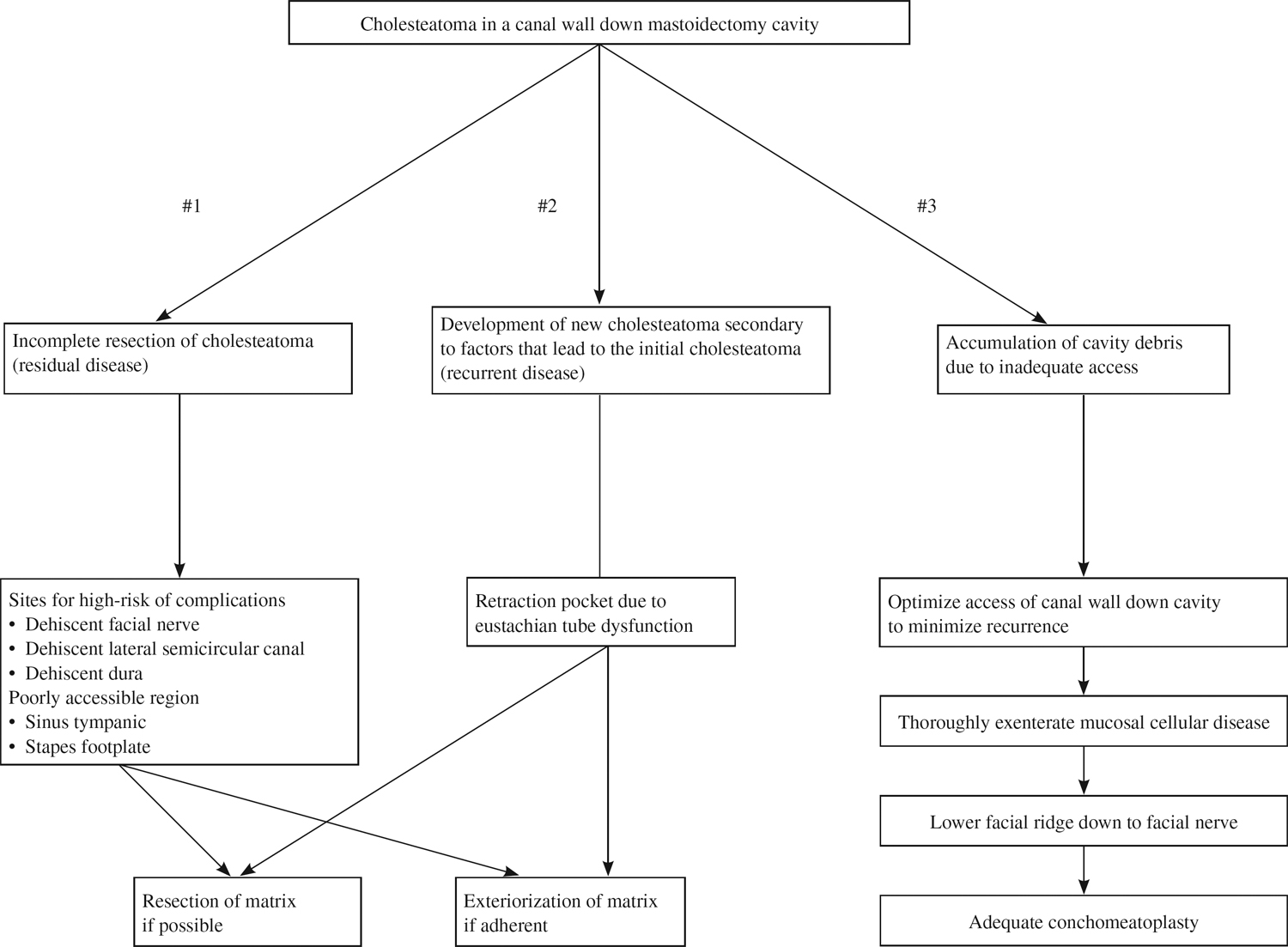
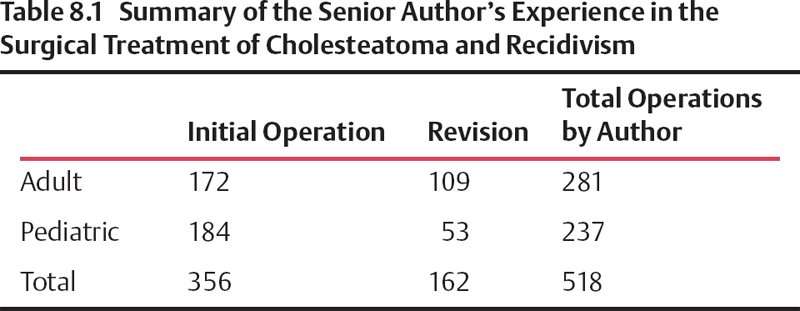
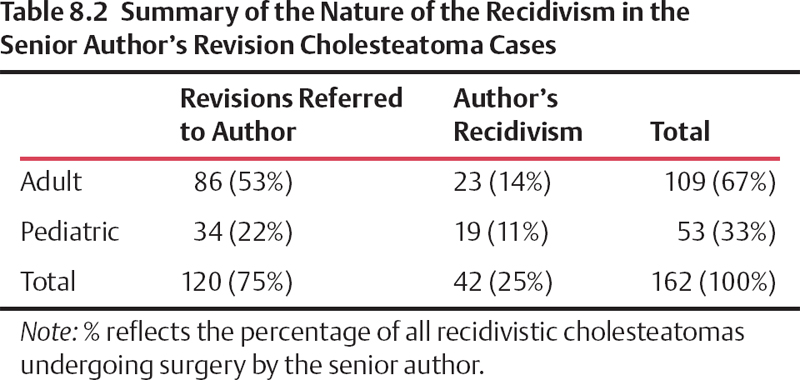
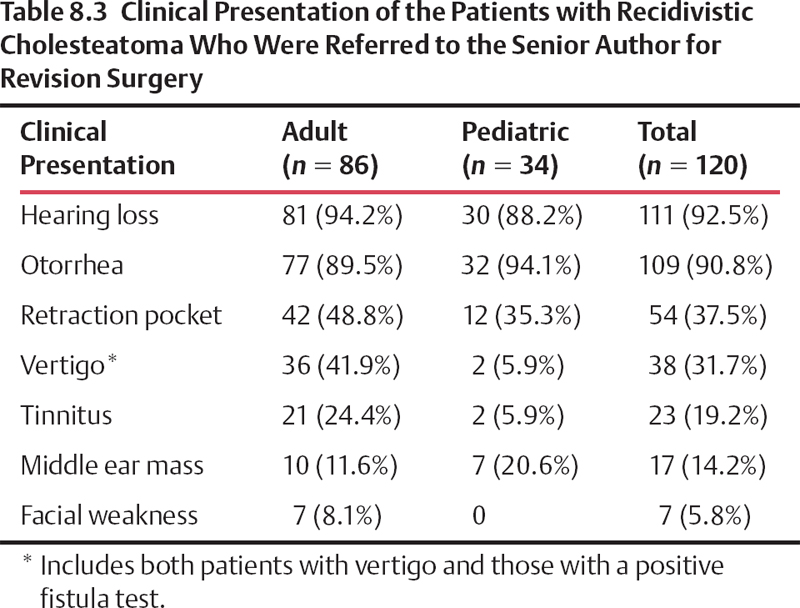
8 Revision Surgery for Cholesteatoma or Chronic Otitis Media The primary goal of surgery for cholesteatoma is complete eradication of the disease process. Additionally, the surgeon seeks to preserve or restore hearing and to provide the patient with a trouble-free dry ear.1,2 Revision surgery presents the otologic surgeon with special problems.3,4 Landmarks frequently have been distorted by the disease process as well as by the prior surgery. Also, patients who have recidivistic disease tend to have the most severe form of chronic ear disease, with poor eustachian tube function and failure of middle ear ventilation. This chapter reviews the experience gained in the diagnosis and treatment of recidivistic cholesteatoma in 162 ears. Highlights of the surgical technique will be discussed. Results in adults and children with respect to production of safe, dry ear, along with hearing results and rates of recidivism, will be reviewed. The causes of failure in surgery for cholesteatoma may be incomplete resection of the disease (residual disease) and poor surgical technique, but the cause may also be a severe form of chronic ear disease with poor eustachian tube function or the failure of middle ear ventilation (recurrent disease). In our hands, the rate of recidivism (whether recurrent or residual disease) is 11% in the pediatric population and 14% in the adult population. These numbers vary greatly between different centers and different surgeons with varied approaches to the treatment of chronic otitis media with cholesteatoma. The following are the highlights of our surgical technique in treating recidivistic cholesteatomatous disease. In patients who have had a skillfully performed canal wall down operation, a residual cholesteatoma may present as a localized “pearl” in the mastoid and can be marsupialized in the office. The area is anesthetized either with a 50% topical phenol solution or by use of local anesthetic infiltration. The lateral wall of the cyst is excised, and the keratin accumulation is aspirated. The epidermal base is preserved, and, having been unroofed, it will form a stable skin lining. Residual disease localized within the middle ear cleft will usually require only a tympanotomy for removal, but if the disease has extended into the sinus tympani, its removal will be more difficult. To expose this area, the bone anterior and lateral to the vertical portion of the facial nerve must be removed. Exposure of this area may be facilitated by performing a canal wall down mastoidectomy. An alternative is to perform an extended hypotympanotomv via a canal wall intact mastoidectomy, preserving the posterior canal wall. This procedure will increase exposure of the sinus tympani, but not to the degree obtained in a canal wal1 down approach. Isolated residual disease within the mastoid cavity following an intact canal wall procedure occurs relatively infrequently. In such cases, performing a revision mastoidectomv will allow for its complete removal. The mastoid cortex may have regenerated, especially in children. If the mastoid has adequate aeration after the initial procedure, the surgeon may find an otherwise air-filled, mucosa-lined cavity, and the disease can be removed and the canal wall preserved. However, when residual keratinizing epithelium invades air cells, it may insidiously grow extensively within the temporal bone. Its removal will require meticulous exenteration of the remaining “accessible cells,” a process that can be time consuming and technically demanding. Even in large, cellular mastoids, sacrificing of the posterior canal wall may be required to obtain the necessary exposure to permit the complete removal of existing disease when the pathology is found to be clinically more aggressive, as in massive cholesteatoma regrowth. Recurrent disease is a frequent problem in intact canal wall cholesteatoma surgery.5 Recurrent disease occurs when the underlying eustachian tube function is inadequate to equalize pressures within the middle ear mastoid complex. It must be recognized that removal of middle ear or mastoid disease will not affect disorders intrinsic to the eustachian tube. Regretfully, otologists are not able to predictably evaluate or to improve the physiologic function of the eustachian tube, even though nasal, nasopharvngeal, and sinus disease may have been successfully treated. Effective eustachian tube surgery or treatment that improves tube function has not yet been developed. Thus, following canal wall up surgery, recurrent cholesteatomas may develop. Decision tree for cholesteatoma Marsupializing the mastoid into the ear canal eliminates it as an air-containing cavity and precludes the need for ventilation. A canal wall down procedure provides an unobstructed exposure of the middle ear, anterior epitympanic-zygomatic area and may facilitate eradication of disease from the sinus tympani. When a patient with a cholesteatoma develops a labyrinthine fistula or a significant intracranial complication in an ear having had a canal wall up procedure, it is essential to convert it to a canal wall down mastoidectomy. Often, a patient with localized erosion from an attic cholesteatoma, or with a prior limited atticotomy, will present with an epitympanic retraction despite a well-aerated middle ear. In such ears, the loss of underlying bony support may have led to a collapse of the overlying keratinizing epithelium. If canal skin collapses onto the floor of the epitympanum, it may block mastoid aeration. The attic defect progressively retracts behind the posterior canal wall into the antrum, producing a recurrent cholesteatoma. One may suggest that removal of the retraction and reconstruction of the lateral epitympanic wall with a cartilage graft could eliminate the problem. However, if there is poor eustachian tube function, over time recurrent disease may still develop in some of these reconstructed ears. Revision surgery is indicated in the treatment of recidivistic disease whether due to recurrent or residual cholesteatoma. The clinical data from the senior author’s experience with 518 ears operated upon for cholesteatoma were reviewed. Three hundred fifty-six were primary cases, 172 (48%) adults and 184 (52%) children. Recidivistic cholesteatoma accounted for 162 (31%) of the total cases (Table 8.1). Fifty-three (10% of total patients) were children, and 109 (21% of total patients) were adults. Half of the adult cholesteatomas occurred in males, whereas in children males accounted for 65% of patients. Right and left ears were affected equally. The mean age for the adults was 42.6 ± 15 years and for children was 8.6 ± 4.7 years. The patients with cholesteatoma regrowth in this series can be subdivided into two groups (Table 8.2). The first is composed of 120 ears initially operated elsewhere and referred to the senior author for treatment of recidivistic disease. The second is composed of 42 cases of cholesteatomatous regrowth in ears previously operated on by the senior author. These were analyzed separately. Many of the patients in this latter group were asymptomatic, the regrowth being discovered during the course of office follow-up examinations. The following parameters were analyzed: presenting signs and symptoms of recidivism, interval of time between initial surgery and diagnosis of recidivism, types and incidence of complications in the recidivism group, and results of revision surgery. The regrowth of a cholesteatoma produced symptoms similar to those produced by the original disease (Table 8.3). Drainage and hearing loss were the most commonly observed symptoms. Usually, there was a recurrence of foul-smelling otorrhea in a previously dry ear and a deterioration in hearing. Otalgia occurred quite frequently in children (41%) and was less common (19%) in adults. Episodes of vertigo were commonly reported by adults (42%) but rarely in children. Eight percent of adults with cholesteatoma regrowth presented with a facial nerve paralysis, whereas no children in this series suffered this disfigurement. Regrowth of cholesteatoma occurred regardless of the type of initial procedure performed (Table 8.4). Patients having had a closed, canal wall up technique developed both residual or recurrent cholesteatoma and cholesteatoma of unknown origin (Table 8.5
Causes of Failure of Primary Surgery
Revision Surgery
Surgical Technique for Residual Cholesteatoma
Recurrent Cholesteatoma
Indications for Revision Surgery
Presenting Symptoms
Otologic Findings
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Revision Surgery for Cholesteatoma or Chronic Otitis Media
