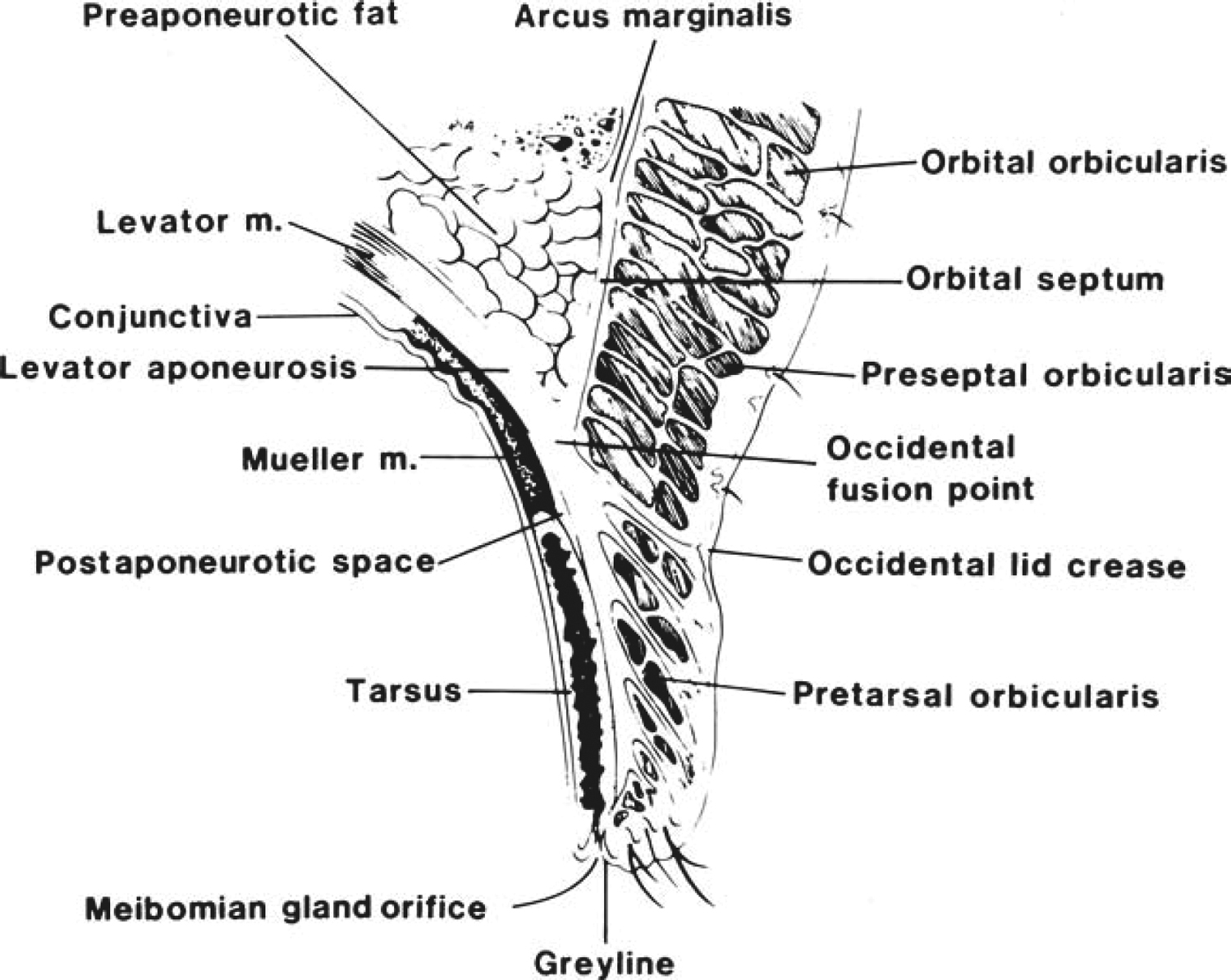
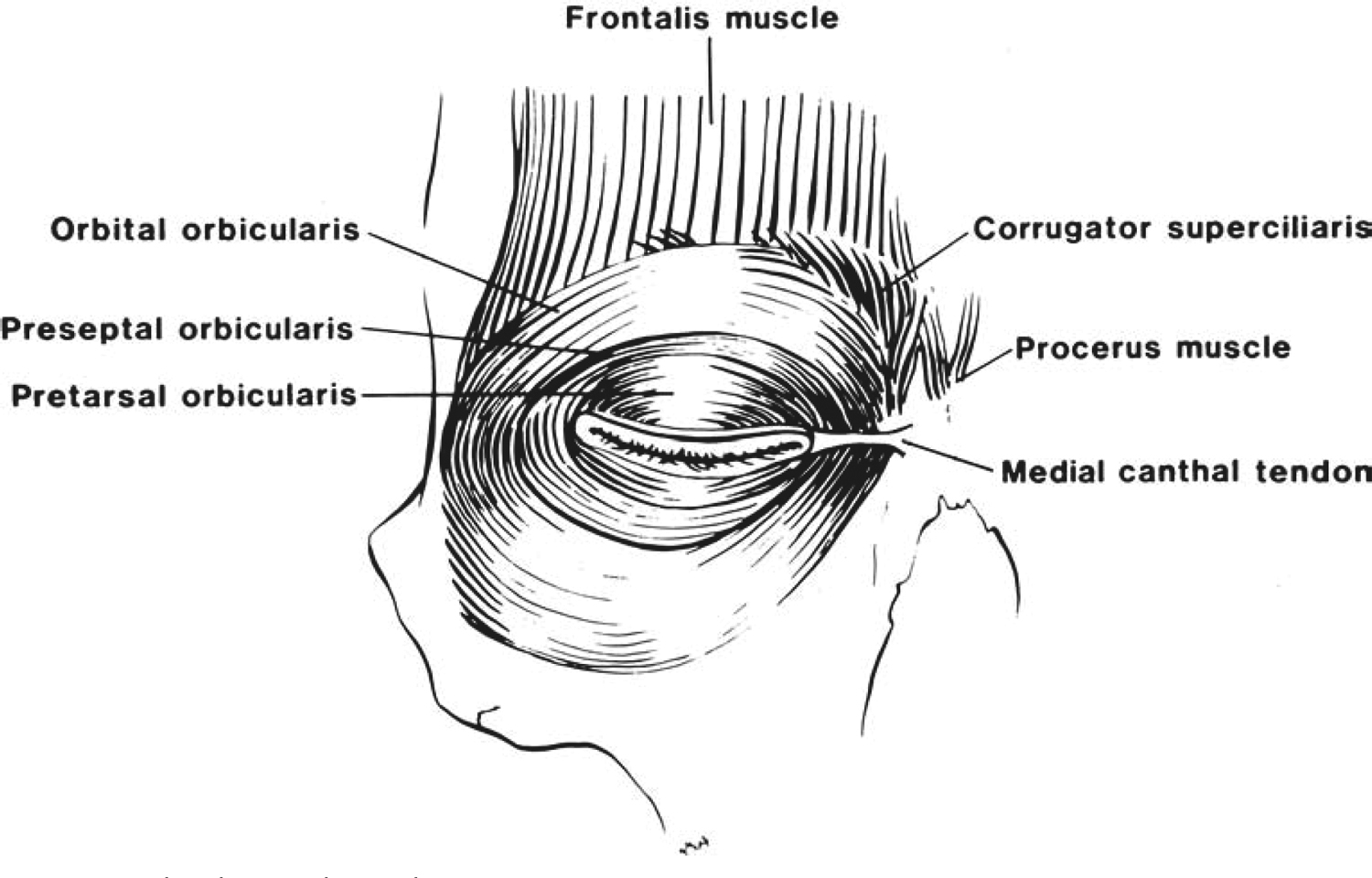
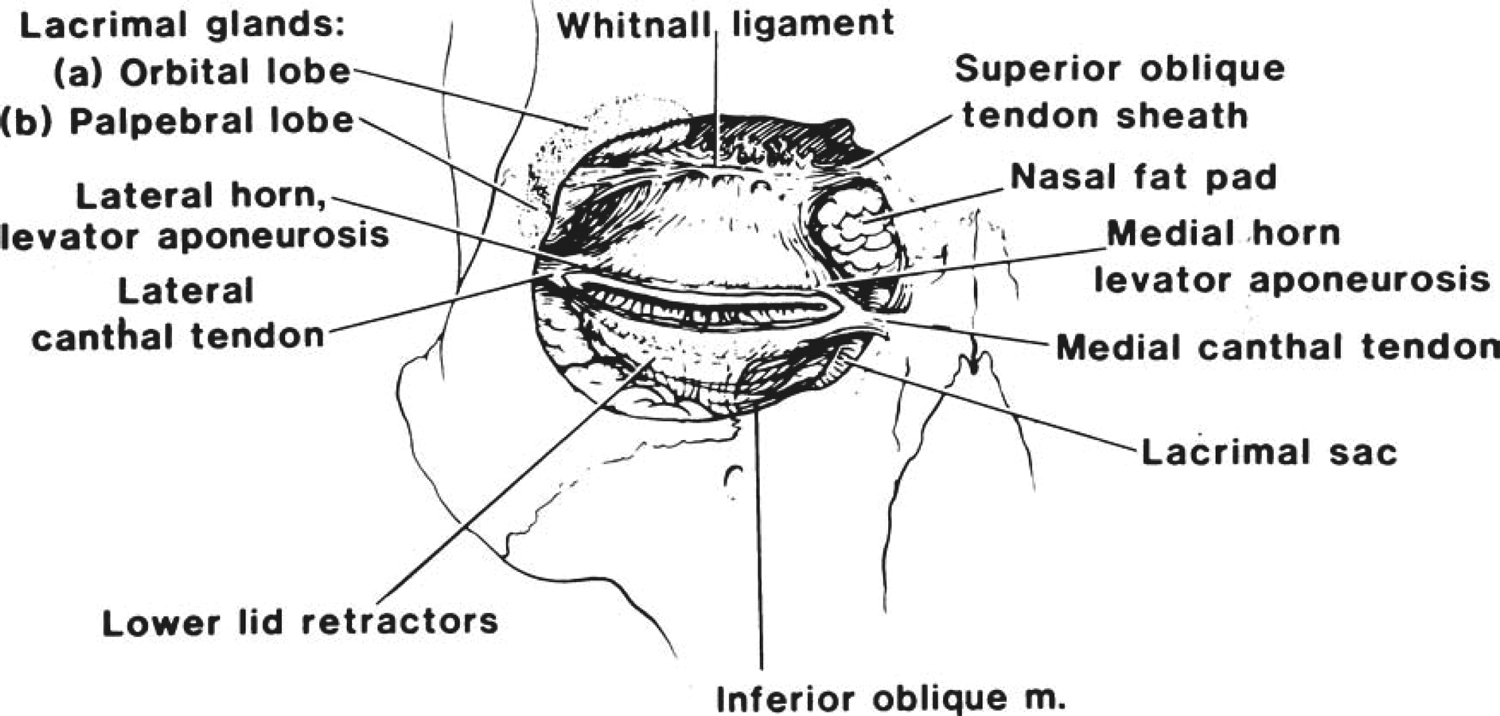
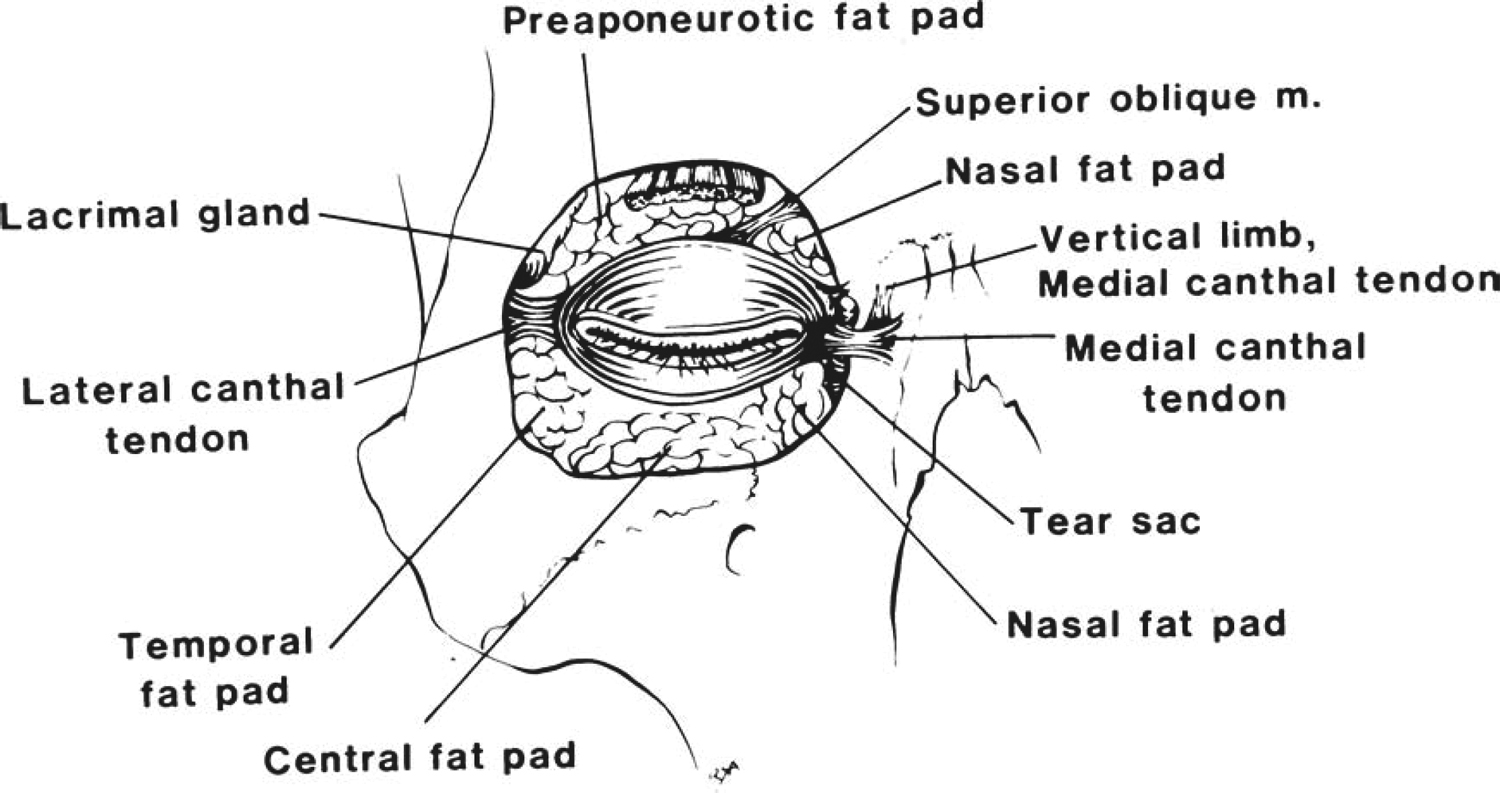
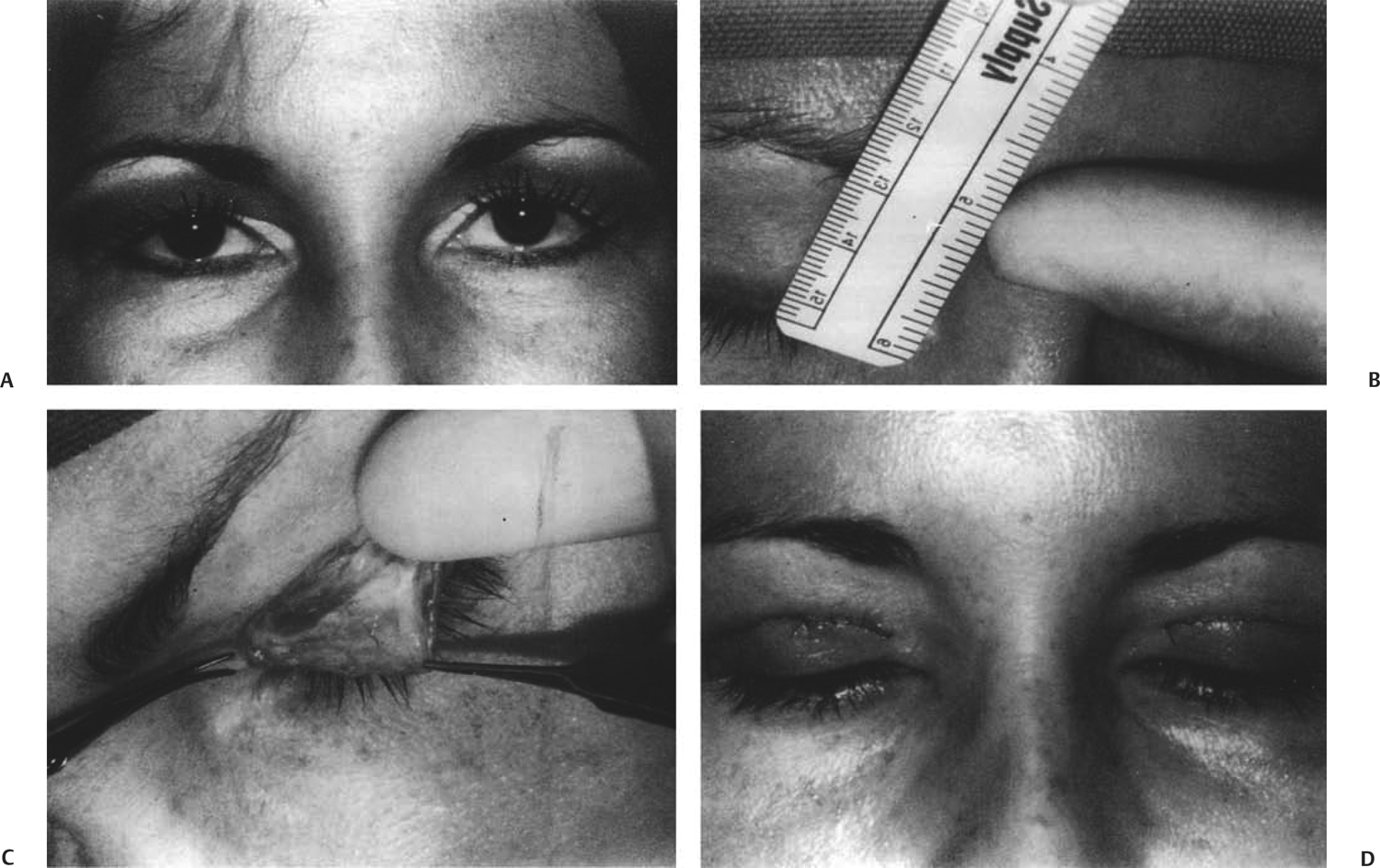
32 Revision Surgery for Blepharoplasty This chapter reviews the main anatomical structures involved in eyelid surgery. It discusses complications of upper and lower blepharoplasty and outlines surgical techniques addressing undercorrection, high or asymmetric eyelid creases, nasal tension lines, suture milia, superior sulcus syndrome, feminization of the male eyelid, ptosis secondary to upper eyelid blepharoplasty, lagophthalmos, bleeding, lower eyelid retraction, lateral tarsal strip and horizontal lid shortening, long-standing or severe lower eyelid retraction and lower eyelid ectropion, under- or overexcision of lower eyelid fat, and postoperative skin wrinkling. The eyelids are the main protection mechanism for the globe; therefore, it is not difficult to understand why ophthalmic complications can result from any type of eyelid surgery. The eyelids consist of the anterior lamella of skin and orbicularis muscle and a posterior lamella of tarsus and conjunctiva. The precorneal tear film is composed of three layers. The superficial lipid layer is produced predominantly by the meibomian glands and the glands of Zeis and Moll, which aid with lubrication of the cornea by dispersion of the tear film and retardation of tear film evaporation. Any disturbance in the position of the margin or change in palpebral fissure height can precipitate a disturbance in the ocular surface. The interpalpebral fissure is the exposed zone between the upper and lower eyelids. The normal adult fissure is 27 to 30 mm long and 8 to 11 mm wide. The upper eyelid is more mobile than the lower and can be raised 15 mm by the action of the levator muscle. The frontalis muscle can contribute an additional 2 mm, and the orbicularis oculi muscle is the levator’s antagonist. In the adult the upper eyelid rests 1.5 to 2.0 mm below the upper limbus, with the highest point of the lid contour slightly nasal to the pupil. The lower lid is positioned at the lower limbus, with the lowest point of the lid contour slightly temporal. The junction points where the upper and lower eyelids meet are the commissures; the angles the lids form are the canthi. The upper eyelid crease is most commonly found 8 to 10 mm above the upper lid margin in occidental eyelids. The crease represents insertion of levator fibers in the pretarsal orbicularis and skin. The eyelid crease in Asians is only a few millimeters from the upper lid margin because the superior orbital septum inserts on the levator aponeurosis at the crease, close to the lid margin. The area of skin above the cilia in which the skin and underlying muscle are firmly attached to the tarsal plate is the pretarsal space. The visibility of the pretarsal space is dependent on the amount of skin overhanging the upper lid fold (dermatochalasia). The goal of upper lid blepharoplasty is restoration in the visibility of the pretarsal space, more so in females than in males (Fig. 32.1). If the medial canthus is covered by a nasal extension of the upper lid crease, this is termed an epicanthal fold. The lower eyelid crease is less well defined and represents the superficial insertion of the lower lid retractors. The crease is 4 to 5 mm below the lower eyelid margin and has a gradual temporal slope. The eyelid skin is the thinnest in the body and makes a sharp transition to the thick skin of the brow superiorly and the malar region inferiorly. The subcutaneous tissue in the eyelids is devoid of fat and has loose stroma and attachments to the underlying tissue. This explains the rapid accumulation of fluid in the pretarsal space during hemorrhage or acute allergic response, with an initial sharp demarcation line between the cheek region. The orbicularis oculi muscle is deep to the dermis and is the protractor of the eyelids (closure muscle). It is divided into three regions: the pretarsal, preseptal, and orbital regions (Fig. 32.2). The pretarsal orbicularis divides into two heads nasally. The superficial head passes anterior to the canaliculi and forms the anterior crus of the medial canthal tendon, inserting into the frontal process of the maxillary bone. The deep head inserts onto the posterior lacrimal crest (Horner muscle). This deep insertion provides a deep anchor and is responsible for the eyelids’ convex position on the surface of the globe. The preseptal orbicularis medially inserts into the anterior crus on the medial canthal tendon and temporally forms the lateral horizontal raphe. The orbital orbicularis nasally inserts into the medial canthal tendon, the nasal aspect of the frontal bone, and the inferomedial orbital margin. It then extends laterally around the lateral canthus without insertion into the lateral canthal tendon. The orbicularis muscle provides the lacrimal pump for drainage of tears into the nasolacrimal system. Weakening of the muscle can cause epiphora even in the presence of normal lid position. Fig. 32.1 Cross-sectional anatomy of the upper eyelid. Deep to the orbicularis muscle is the orbital septum, which is firmly adherent to the arcus marginalis of the orbital rim. The septum inserts medially to the posterior lacrimal crest and lacrimal fascia. Laterally, the septum is attached to the lateral canthal tendon and the lateral orbital tubercle. Anteriorly, the orbital septum forms a barrier for the orbital tissues and prevents anterior displacement of the orbital fat. Fig. 32.2 Orbicularis oculi muscle. Fig. 32.3 Orbital septum and associated structures. In the lower eyelid, the septum fuses with the lower eyelid retractors 4 to 5 mm below the tarsal plate, then attaches to the inferior border of the tarsus of the lower lid. In the upper eyelid, the septum fuses with the levator aponeurosis superior to the tarsal plate, ~10 mm above the eyelid margin in occidental eyelids. In Asians, the orbital septum inserts to the levator aponeurosis anterior and inferior to the tarsal plate only a few millimeters from the eyelid margin (Fig. 32.3). The preseptal eyelid fat pad extends in a submuscular plane from the brow region inferiorly beneath the preseptal orbicularis of the upper eyelid. In the upper eyelid posterior to the orbital septum are two fatty compartments. The preaponeurotic fat pad lies anterior to the levator aponeurosis, temporal to the trochlea, and medial to the orbital lobe of the lacrimal gland. Nasal to this fat pad is the nasal fat pad of the upper lid just beneath the trochlea. These fatty deposits can be discerned by their color; the preaponeurotic fat pad is yellow, whereas the nasal fat pad is white. In the lower eyelid there are three fat pads. The inferior oblique muscle divides the nasal and central fat pads. The central and lateral fat pads are divided by a fibrous septum anteriorly but connected in the deep tissue posteriorly (Fig. 32.4). The most common complication of cosmetic blepharoplasty is dissatisfaction with the surgical results. The easiest way to avoid this complication is by spending time during the preoperative visit explaining to the patient what can be expected. Preoperatively, the patient must be advised of all potential cosmetic outcomes of upper blepharoplasty. including under- and overcorrection, high eyelid creases, asymmetry, nasal tension lines, suture milia, superior sulcus deformity, and feminization of the male upper eyelid. The patient must have realistic expectations even if the procedure progresses as planned. More importantly, the patient must be advised of the functional complications that require surgical revision, including ptosis, hematoma, lid lag or the inability to close the eyelids when sleeping, exposure keratopathy, and vision-threatening retrobulbar hemorrhage. Common complications of lower blepharoplasty are fewer and more accentuated than those of upper blepharoplasty. Cosmetic and functional complications include lower lid malposition, retraction with scleral show (Fig. 32.5), ectropion, lagophthalmos, bowing deformity, injury to the inferior oblique muscle, worsening of rhytides, improper orbital fat excision, accentuation of the tear trough deformity, and orbital hemorrhage. Fig. 32.4 Orbital fat compartments. The desired cosmetic result of upper blepharoplasty is a tall, exposed anterior surface of the upper eyelid skin, yielding a youthful appearance. The most common cosmetic complaint of patients is underexcision of skin or dermatochalasia. This complication is very amenable to reoperation, with excision of skin and orbicularis muscle above the previous incision. If the lid crease height is appropriate, the reoperation incision can be made through the original incision along its entire length, maintaining the lid crease height. Additional orbital fat can be excised to reduce residual bulges, most commonly remaining at the medial fat pad. The skin is then reapproximated, as would any blepharoplasty incision, with interrupted, running, or subcuticular sutures. If the lid crease requires enhancement, the underlying levator aponeurosis is incorporated into each pass of the needle. Fig. 32.5 Asymmetric lid creases after blepharoplasty. A common complication of upper eyelid blepharoplasty is inappropriate placement of the upper eyelid crease, most commonly an exaggeratedly high lid crease. This can be a difficult complication to repair, and in cosmetic blepharoplasty it should be avoided, especially in males. A high eyelid crease yields a feminine appearance, and this should be addressed preoperatively in male patients. Maintaining the height of the patient’s preoperative eyelid crease height is the best way to avoid this complication unless the patient already has asymmetric eyelid crease height or levator aponeurosis dehiscence with an elevated lid crease. The surgeon should always err on the side of placing the lid crease too low rather than too high, as this is more easily repaired. The eyelid crease, as previously mentioned, represents the insertion of the levator fibers into the pretarsal orbicularis and skin. To lower the crease surgically, a new blepharoplasty incision should be placed at the desired lid crease height (usually 8–10 mm superior to the eyelid margin). The incision should be carried down through the orbicularis muscle and orbital septum to the levator aponeurosis. If required, a skin–muscle flap and herniated orbital fat may be removed. The incision is then closed with interrupted sutures. The sutures reestablish the new lid crease, as each suture pass incorporates the inferior incisional skin edge and a bite of levator aponeurosis and then the superior skin edge, imbricating the aponeurosis within the skin closure. This allows the upper eyelid skin to slightly hang over the closed incision, re-creating the upper eyelid crease. It should be stressed that taking too much skin laterally in reoperations should be avoided, as it will pull the eyebrows inferiorly. Fig. 32.6 (A) Patient following upper lid blepharoplasty. Note the iatrogenic asymmetric, low eyelid creases. (B) The lid creases are almost touching the lashes. On measurement, the lid crease is 4 mm above the lash line. (C) To repair the low lid crease, a skin–muscle flap is dissected below the previously formed lid crease. (D) Postoperative appearance after reformation of the lid creases. Note the newly elevated, symmetric lid creases. Asymmetric upper eyelid creases are also encountered after blepharoplasty; this asymmetry is more easily corrected by elevating the eyelid crease that is too low (Fig. 32.5). The distance from the lid margin to the lid crease in the eye that is not to be repaired is measured. An ellipse of skin is marked on the eyelid to be repaired above the existing lower eyelid crease, with the inferior incision placed at the same height as the lid crease measured on the opposite eye. The marked ellipse is then excised as a skin–muscle flap along the horizontal length of the eyelid, and levator aponeurosis adhesions are separated from the previous lower eyelid crease. The incision is closed in a similar manner as mentioned above, with interrupted sutures incorporating the levator aponeurosis into the newly repositioned eyelid crease. The inferior and superior incisional suture passes should be orbicularis and skin together, enhancing the lid crease (Fig. 32.6). Nasal tension lines or nasal webbing can be avoided with a W or M incision configuration; however, mechanically created nasal tension lines can also occur during incision closure (Fig. 32.7). This can be prevented primarily if tension is noted at the time of suturing. The first pass of the running suture should be placed lateral to the most nasal incision angle (~4 mm), taking a bite of skin and orbicularis inferiorly, then the levator aponeurosis, and then in a parallel vector through skin and orbicularis superiorly (instead of at a meridianal angle). This creates lateral tension on the upper nasal eyelid skin, reducing tension lines. No sutures should be placed medial to the first pass of the running suture. If tension lines are still present, remove the first stitch of the running suture and place it even more temporally, again leaving the incision open nasal to the running suture. Fig. 32.7 Nasal tension lines after blepharoplasty. Fig. 32.8 Suture milia after blepharoplasty. Suture milia are incisional cysts at the area where the suture passes into the skin (Fig. 32.8
Anatomy
Superficial Anatomy
Skin and Muscle
Orbital Septum
Preseptal and Postseptal Eyelid Fat Compartments
Complications of Blepharoplasty
Complications of Upper Blepharoplasty
Complications of Lower Blepharoplasty
Surgical Revision for Upper Blepharoplasty
Undercorrection

High or Asymmetric Eyelid Creases
Nasal Tension Lines

Suture Milia
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


