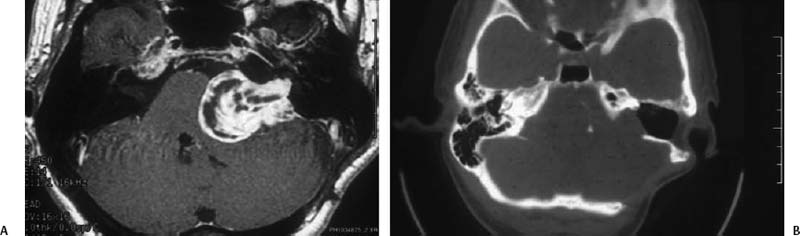
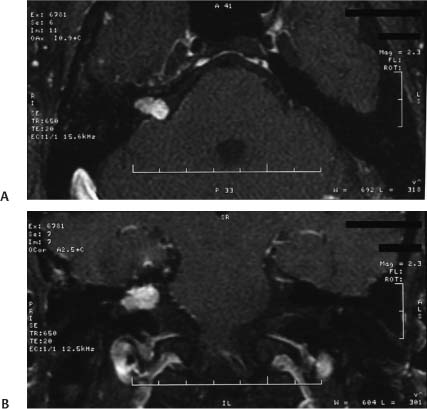
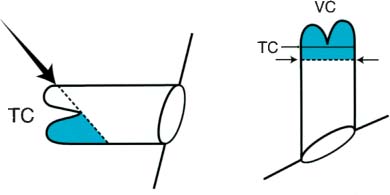
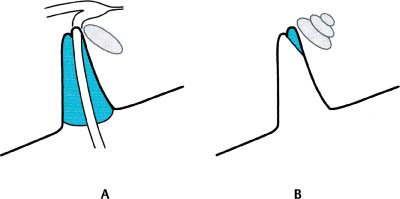
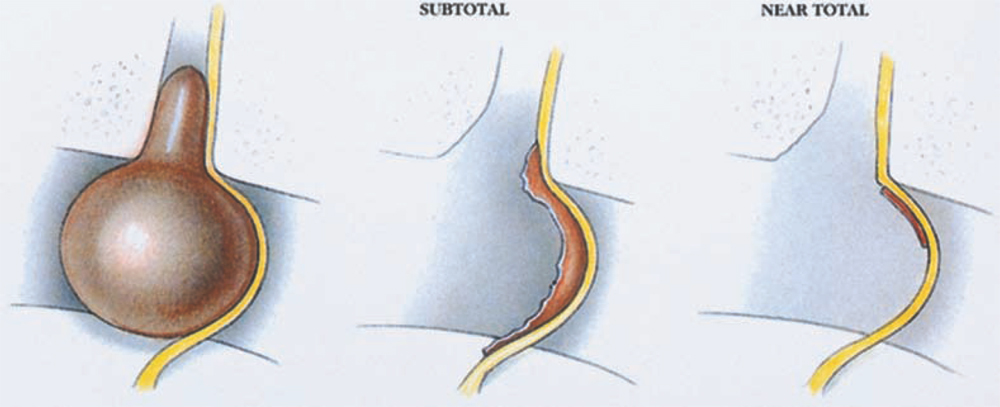
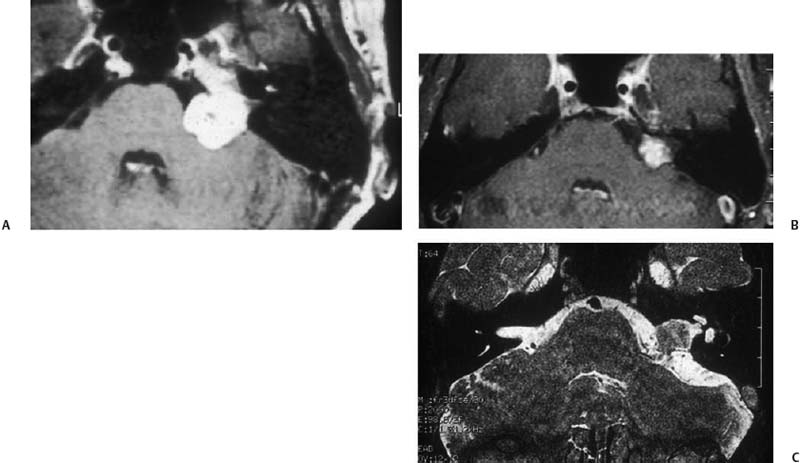
10 Revision Surgery for Acoustic Neuroma The goals of vestibular schwannoma (VS) treatment have differed at various times in history. In the early 1900s, Harvey Cushing recommended intracapsular enucleation with no effort made to achieve complete tumor removal.1 Later, Walter Dandy, a former student of Cushing, proposed that complete tumor removal should be the goal.2 After the introduction of the microscope, modern surgical techniques, and the concept of a skull base team, complete tumor removal became the objective, and virtually all tumors were operated soon after discovery. In general, the philosophy of complete tumor removal persists today but not without some important exceptions. The management of acoustic neuromas is becoming increasingly complex because of early identification (very small tumors), a better understanding of tumor growth (or lack thereof in some patients), hearing conservation operations, the concept of a near total removal, and the now widespread availability of stereotactic radiosurgery (SRS). Recurrence of VS after apparently complete microsurgical resection with modern techniques is rare. SRS also appears to result in long-term tumor control in the majority of patients. When a recurrence is detected after microsurgical removal, or tumor progression occurs after SRS, the management paradigm is different than that for primary tumors. In this chapter, we will review the frequency of tumor recurrence after treatment by SRS and microsurgery, the causes of failure, treatment options, and surgical technique. The definition of recurrent tumor varies among studies. For some authors, only tumors that were thought to be completely resected at the primary surgery and then subsequently regrow are considered a true recurrence. Tumors that were knowingly incompletely removed (e.g., small residual in the fundus or along the facial nerve) are termed residual tumors. In this chapter, unless otherwise specified, we use the term recurrence broadly to include residual tumors and to describe tumor regrowth in the setting of what was thought to be complete removal. Because of the different pathophysiology, patients with neurofibromatosis type 2 (NF2) are not included by most authors in calculating recurrence rates. The overall published recurrence rate after complete microsurgical tumor removal is quite low, 1 to 2% in most studies.3 These studies, however, most likely underestimate the true recurrence rate for several reasons. First, there is a lack of sufficient long-term radiologic follow-up with magnetic resonance imaging (MRI) scans to exclude late or very small recurrences. Second, patients with recurrent tumors often seek care at an institution other than that providing the original surgery. Third, asymptomatic patients may not continue to return for follow-up. These patients may have radiographic evidence of recurrent or residual tumors but are without symptoms.The clinical presentation of recurrent tumors is different than that of primary tumors because the hearing that may have been present originally has most often been lost after the initial surgery. Although many tumors are discovered during routine postoperative surveillance,a significant number of patients are lost to follow-up or told they are cured after a short follow-up period. Beatty et al reported on 23 patients who underwent revision surgery for recurrent tumors; the most common symptoms at the time of reoperation were ataxia, facial paresthesias, and headaches.4 Figure 10.1 shows a large recurrence after a retrosigmoid resection in a patient who opted to avoid follow-up examinations or imaging for financial reasons. A VS recurs either because the tumor was left unresected or because a new tumor has grown de novo. Patients with NF2 fall into this second category, and the tumor recurrence in these cases may not represent a technical failure with the primary treatment modality but may simply reflect the natural history of the disease. These patients should be considered separately. Most recurrences occur because the surgeon either chose to leave the tumor unresected (near-total or subtotal removal) or inadvertently failed to extirpate all tumor due to the inherent technical challenges of the operation. A few general statements about recurrences can be made. First, if the surgical team is experienced and a complete gross tumor removal is achieved, the recurrence rate is very low. Second, if a tumor recurs after “complete removal,” it will most likely do so in the lateral end of the internal auditory canal (IAC). Third, subtotal resections often grow and require further treatment.5,6 Fig. 10.1 (A) Axial T1 postgadolinium magnetic resonance imaging showing a large cystic recurrence approximately 10 years after “complete” removal via the retrosigmoid approach. The patient had refused any follow-up imaging after the primary surgery. She underwent a revision surgery again via the retrosigmoid approach. Subsequent postoperative imaging demonstrated another recurrence in the fundus of the internal auditory canal. (B) Axial computed tomography scan following resection of the second recurrence through the translabyrinthine approach. Because the tumor was restricted to the internal auditory canal, limited bone removal was needed to fully expose the tumor and achieve complete removal. Note the remaining bone along the posterior face of the petrous bone medial to the sigmoid sinus. It appears from the literature that the recurrence rate may vary slightly depending on the surgical approach used. For surgeons familiar with all three common surgical approaches, the retrosigmoid (RS), translabyrinthine (TL), and middle fossa (MF), it is not surprising that the TL approach has the lowest apparent recurrence rate. There is little argument that this approach affords the best visualization of the lateral end of the IAC, the site of most recurrences. A large series from the House Ear Clinic (3123 patients) found a recurrence rate of 0.3%, excluding patients with NF2 and those with incomplete tumor removals.7 The average time from the initial tumor removal to recurrence was 10 years, underscoring the importance of long-term follow-up. Although not specifically stated, it is probable many of these patients were followed radiologically with computed tomography (CT) scans. Had MRI technology been available, the elapsed time to identification of a recurrence would likely have been less. In a large series of 620 tumors removed via the RS approach, without an attempt to preserve hearing, three patients (0.5%) developed a recurrence.8 The same authors reported a recurrence rate of 1.5% (4/260) when an attempt was made to preserve hearing through either an RS or MF approach. Many smaller studies with various follow-up ranges and inclusion criteria and surgical approaches report recurrence rates ranging from 0 to 7.5%.3,5,8 The rate of 7.5% is in a series of 83 tumors thought to be completely removed via the MF or extended MF approach. Three of the six patients were reoperated, and recurrences have been confirmed while the other three patients were being followed by serial imaging. The lateral extent of the tumor is often not directly visible during the RS or MF approach. In the RS approach, the preserved overhanging bone of the otic capsule structures precludes direct visualization of the fundus of the IAC. The tumor remnants must be dissected blindly with angled instruments or with the use of an endoscope. Not surprisingly, the risk of recurrence is higher in this approach compared with the TL, where the entire distal IAC is routinely visualized.9 If hearing preservation is not a priority during the RS approach, then the lateral end of the canal can be exposed completely, obviating the need for any blind dissection. The MF approach provides its own unique exposure challenges. Fig. 10.2 depicts a recurrence after the MF approach. In the MF approach, a tumor in the fundus may be obstructed from direct view by the transverse crest and by the facial nerve (Figs. 10.3, 10.4). Approximately 25% of the inferior wall of the IAC is not directly visible during the MF approach.10 Awareness of this anatomy and proper instrumentation are essential to achieving complete tumor removal. Lastly, there will be occasional cases with tumor extension into the cochlea; even with the TL approach, this type of tumor may be left behind.11,12 In summary, all the approaches present anatomical limitations that may increase the risk of incomplete tumor removal. Because the risk of recurrence after microsurgery is overall very low, it is our opinion that this variable should not be a significant consideration in choosing a surgical approach. Other issues, such as tumor size and location, hearing status, facial nerve outcome, postoperative headache risk, and cerebrospinal fluid (CSF) leak, will have a greater impact on our choice of approach than the risk of recurrence. Fig. 10.2 (A) Axial and (B) coronal MRI scan postadolinium depicting a recurrence after the middle fossa approach. Occasionally, a muscle plug used to fill the defect after the primary surgery will enhance and be mistaken for recurrent tumor. We now use a small fat graft that can easily be distinguished from recurrent tumor using fat suppression algorithms. Serial images demonstrated tumor growth, confirming it as a true tumor recurrence. Fig. 10.3 (A) Arrow indicates the surgeon’s angle of view to the internal auditory canal; shaded area indicates the tumor hidden from direct view by the transverse crest (TC). (B) View of the internal auditory canal from a superior position; shaded area represents a hidden tumor. VC, vertical crest. (From Driscoll CLW, Jackler RK, Pitts LH, Banthia V. Is the entire fundus of the internal auditory canal visible during the middle fossa approach for acoustic neuroma? Am J Otol 2000;21:382–388. Reprinted with permission.) Fig. 10.4 (A) The facial nerve is in a relatively unfavorable location during the middle fossa approach, lying between the surgeon and the tumor (shaded area). However, the nerve in the midportion of the internal auditory canal can be moved from side to side to gain access to the tumor. (B)The shaded area is the tumor located under the immobile portion of the nerve as it exits the canal. Tumor in this location can be difficult to remove atraumatically from the overlying nerve. (From Driscoll CLW, Jackler RK, Pitts LH, Banthia V. Is the entire fundus of the internal auditory canal visible during the middle fossa approach for acoustic neuroma? Am J Otol 2000;21:382–388. Reprinted with permission.) Increasingly, in the literature, there has been put forth the concept of a “near-total” tumor removal (Fig. 10.5). The idea is to leave a tiny fragment of tumor to limit the risk to cranial nerves and vascular structures. Most often this is a small remnant left on the facial nerve just proximal to the porus acusticus, where the tumor is typically most adherent. This fragment should be meticulously trimmed and coagulated with bipolar cautery, to the extent possible without injuring the facial nerve. This strategy is not a substitute for familiarity with the surgical techniques that are needed to achieve total tumor removal. A vernacular, to help with reporting consistency, has been proposed to describe the tumor fragments that are sometimes left behind. Of course, visually quantifying residual tumor is imprecise. We suggest using the term near-total removal when the fragment left is < 5 mm in diameter and no more than 2 mm thick. Larger residuals should be termed subtotal removals. The risk of developing a recurrence after a near-total tumor removal is low. In a recent series, only 1 (3%) of 33 patients who had a near-total removal developed a recurrence versus 6 (32%) of 19 who had a subtotal removal.13 This experience is consistent with other reports summarized below. Vanleeuwen et al reported results of subtotal removal in 73 patients of a total population of 106.14 Of 106 patients, 23% underwent total removal, 8% near-total removal, and 69% a subtotal excision. The decision to leave tumor was made intraoperatively and was based on the perceived risk of injury to the facial nerve and surrounding structures. Follow-up revealed that 20% of the subtotally removed tumors continued to grow and required further surgical treatment. The eventual complication rates in the patients requiring revision surgery were much higher than in the group of patients who underwent complete removal at the primary surgery. Subtotal resection is not recommended by this group as a viable method to achieve lower long-term morbidity.14 Fig. 10.5 The most difficult area of tumor removal is along the facial nerve just medial to the porus acusticus. Tumor may sometimes be left in this area as a compromise to preserve neural function. The resection is termed a near-total removal if the tumor fragment measures < 5 mm in width and 2 mm in thickness. If a larger remnant is left, then it is considered a subtotal excision. To minimize the risk of recurrence, it is important to coagulate the remnant with bipolar cautery. (From Jackler RK. Atlas of Neurotology and Skull Base Surgery. St. Louis: Mosby-Year Book; 1996:Fig. 1–24. Reprinted with permission.) Another study that examined outcomes after near-total or subtotal resection found a very low incidence of tumor growth.15 Out of 20 patients, 19 were followed by CT scan and 1 by MRI for a minimum of 3 years (mean 5 years). No tumor was visible in seven patients, despite known tumor to be present at the end of the case. Tumor regrowth occurred in only one patient, who had a subtotal removal and the highest estimated residual tumor volume of 5 to 7 cm3. Because most of these patients are being followed with CT scans, longer follow-up is needed before definitive conclusions can be drawn. Figure 10.6 is an example of long-term stability of a large residual tumor fragment after subtotal resection. Fig. 10.6 (A) Preoperative axial postcontrast MRI showing a medium-sized acoustic neuroma. Unfortunately, this patient was congenitally deaf in the contralateral ear. She was operated at another institution via the retrosigmoid approach with the intent of performing a subtotal tumor removal. She lost most of her hearing at surgery (class D postoperatively), but the remaining hearing does help with her lip-reading ability. Her residual tumor has been followed for 12 years and has not grown despite its rather large size, as illustrated on a (B) T1 postcontrast MRI and (C) T2 image.
Microsurgery
Incidence of Recurrence after Microsurgery
Reasons for Tumor Recurrence following Microsurgery
The Impact of the Specific Surgical Approach on Risk of Recurrence
Risk of Recurrence following Near-Total or Subtotal Tumor Removal
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


