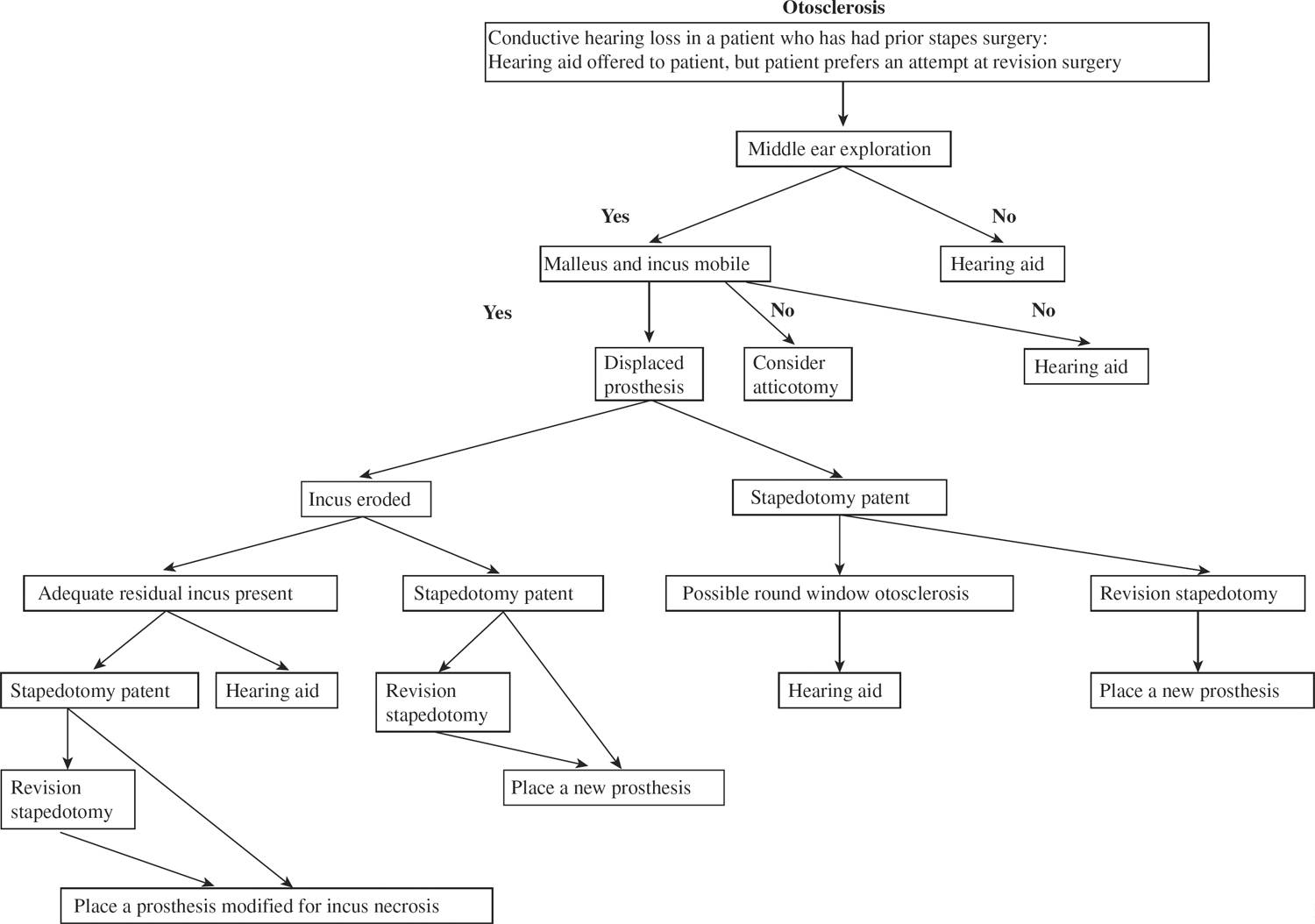
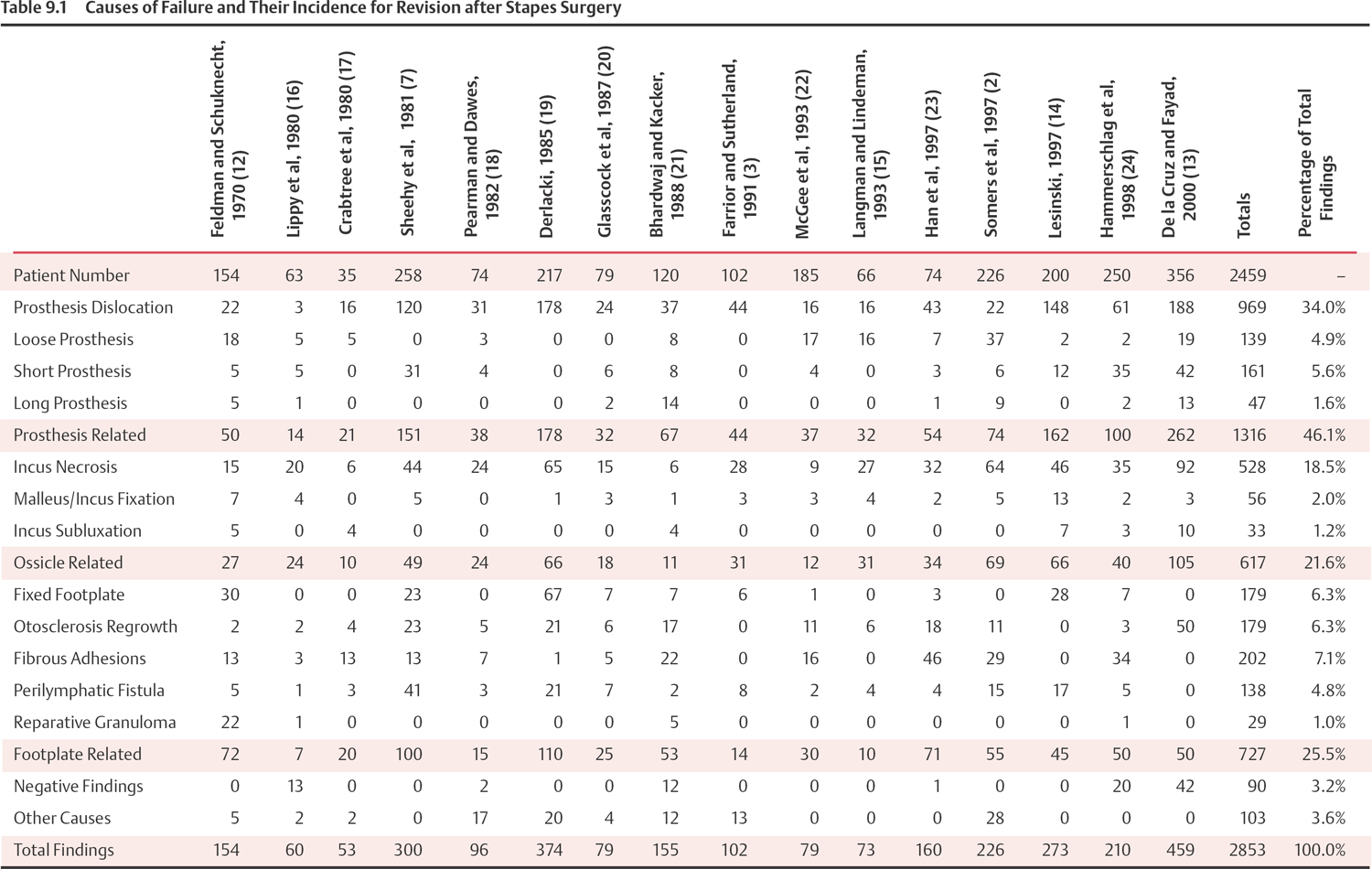
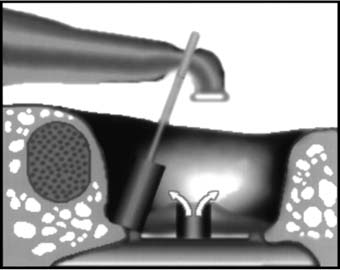
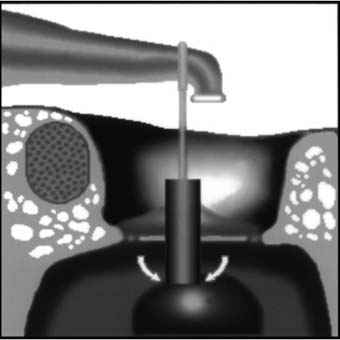
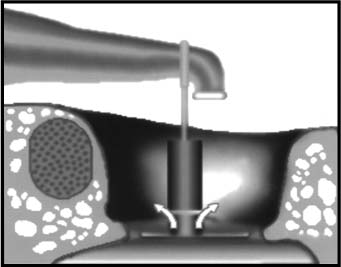
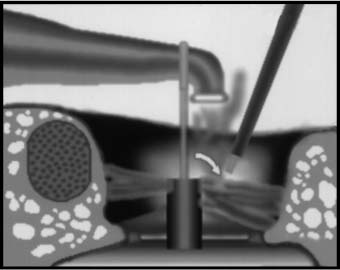
9 Revision Stapedectomy and Stapedotomy Since the reintroduction of stapes surgery in the 1950s, surgeons have come to realize that improved methods for revision stapes surgery must be developed. Revision stapes surgery is not unusual. Some studies estimate that up to 25% of stapes surgeries will require revision.1 Although the literature on revision stapes surgery can be difficult to interpret due to the large variations in patient selection criteria, outcome measures, and operative techniques, some generalizations can be made to help today’s otologic surgeon best treat the revision surgical candidate.2 Because primary otosclerosis is less common now than only a few decades ago, current trends reveal an increased percentage of revision stapes procedures in the overall number of surgeries for otosclerosis.3 Although the exact cause of this decrease in otosclerosis is unknown, many postulates have been offered. Increasing evidence correlates the etiology of otosclerosis to the measles virus, so that the near universal vaccination of children against measles in developed countries may have resulted in the decreased incidence of new cases of otosclerosis noted today.4,5 Further, the addition of fluorides to drinking water may have played a role in the recent fall in incidence.6,7 Finally, because there are fewer primary stapes surgeries being performed, young surgeons have less experience in performing stapes surgery. This may translate into a higher failure rate in primary surgeries, which adds to the increase in the number of revision stapes procedures seen today.8,9 The central issues in revision stapedectomy are the decreased potential for the repair of the conductive component and the increased potential risk of inner ear damage when compared with primary stapes surgery. Outcomes depend on the pathology encountered at revision surgery, as well as the management of the oval window. Technological advances, including the use of the laser, have proved to be important tools in improving hearing results and in decreasing the morbidity of performing both primary and revision stapes procedures. The goal of stapes surgery is to circumvent the inefficient sound transmission of an ossicular chain immobilized by otosclerosis. A group of surgeons from the 19th century, Kessel, Boucheron, Miot, Faraci, and Passow, pioneered procedures intended to mobilize or remove a fixed stapes.5 However, due to the lack of adequate illumination, magnification, and sterile technique, as well as a lack of understanding of the need for oval window and stapes reconstruction, these surgeries often ended in inner ear injury and infection. In 1938, Julius Lempert introduced a one-stage fenestration technique for otosclerosis, bypassing surgery on the stapes.10 He used an endaural approach and a dental drill to create a labyrinthine fenestra, which became the standard for otosclerosis at the time. This procedure was challenged in 1952, when Samuel Rosen reintroduced stapes mobilization for otosclerosis.9 Finally, in 1956, it was John J. Shea’s technique of total stapedectomy that replaced both Lempert’s fenestration procedure and Rosen’s mobilization operation and ultimately became the dominant procedure performed throughout the world for otosclerosis. Shea’s technique involved the removal of the entire stapes, followed by grafting of the oval window with a vein graft. An artificial stapes made of polytetrafluoroethylene (Teflon) was placed on the vein graft in the oval window and attached to the incus.11 Variations have been made in Shea’s procedure in three major areas: the design of the prosthesis, the nature of the oval window seal, and the small fenestration technique. Technological improvements in biocompatible materials, operating microscopes, intraoperative monitoring, and laser tissue vaporization raised stapes surgery to a higher level. A series of Medline literature searches spanning the time period from 1969 to 2001 was performed. The list of search words included otosclerosis, stapes surgery, reoperation, stapedectomy, stapedotomy, and revision. A review of the bibliographies of the studies that were found through this search process was also conducted. The criteria for inclusion in this meta-analysis were studies of a defined group of patients that required revision stapes surgery whose outcomes were measured and whose etiologies for failure of the primary stapes surgery were recorded. Studies selected contained data that could be extracted and pooled with those from other studies. No duplication of patient populations between studies was permitted. Sixteen studies met the selection criteria.2,3,7,12–24 Their data can be seen in Table 9.1. Each study categorized the cause and rate of failures differently. This chapter groups the etiology of failures in three broad categories: prosthesis related, ossicle related, and footplate related. Negative findings at re-exploration and all other causes were pooled. Decision tree for revision stapes surgery Patients who have hearing improvement after primary stapes surgery and who develop a recurrent conductive hearing loss, whether early or late, may be good candidates for revision stapes surgery, whereas patients with the same or worse hearing after the primary procedure have a lower revision success rate.25 The type of stapes operation, prosthesis selection, and oval window management are important in anticipating the possible cause of failure. About 46% of failed primary stapedectomy surgeries are caused by prosthesis-related failures. The prosthesis-related failures can be divided into five main categories: prosthesis dislocation, a loose prosthesis, a short prosthesis, a long prosthesis, and a fractured prosthesis. Prostheses must fit onto the incus tight enough to efficiently conduct sound vibrations, but not too tight as to cause necrosis of the bone. The loose connection of the prosthesis to the incus may be due to inadequate crimping. Over time, the prosthesis may migrate from the oval window to create a recurrent conductive hearing loss or even a perilymphatic fistula (Fig. 9.1). Similar migration occurs when a prosthesis is too short to bridge the distance from the incus to the oval window. Accurate measurements help to avoid this complication, especially when stapedotomy is performed. In stapedectomies, there is a greater margin for error in determining the appropriate length for the prosthesis because the oval window tissue seal can effectively transmit vibrations at different levels in the oval window, just as long as it is in stable contact with the prosthesis. Inappropriate prosthesis length may result in inner ear dysfunction. A prosthesis that is too long may traumatize the saccule (Fig. 9.2); a short prosthesis may not occlude the stapedotomy opening and result in a perilymphatic fistula (Fig. 9.3). Adhesions to the prosthesis may also cause fixation and prevent normal conduction of sound to the inner ear. Using lasers, these adhesions can be lysed without causing significant mechanical trauma to the inner ear (Fig. 9.4). A rare reason for prosthesis malfunction is fracture of the prosthesis itself. Fig. 9.1 Displaced stapes prosthesis. Note evidence of incus erosion at the crimping site. White arrows indicate a perilymphatic fistula. Fig. 9.2 A long stapes prosthesis may injure the saccule. Fig. 9.3 A short piston prosthesis will not engage the stapedotomy and will result in a perilymphatic fistula (white arrows). Fig. 9.4 Adhesions to the stapes piston may be vaporized with a laser to mobilize the prosthesis. About one fifth of stapedectomy/stapedotomy failure is due to incus necrosis or erosion. The cause of incus necrosis may be due to one of two mechanisms. Lesinski proposed a theory of incus necrosis resulting from a prosthesis that has migrated out of the oval window (Fig. 9.1).14 In this situation, the prosthesis becomes fixed against the otic capsule. The vibrating lenticular process is abraded by the immobile prosthesis crimped onto it, eventually leading to erosion and necrosis of the distal incus. Lesinski stated that the risk of complete erosion increases if there is a delay of revision following a recurrence of conductive hearing loss.14 Incus necrosis can also result from an overtightened crimping of the stapes prosthesis, limiting the periosteal blood supply to the lenticular process and causing its ischemic necrosis.1 An uncommon etiology for recurrent conductive hearing loss after an initially successful stapes operation is malleus or incus ankylosis or fixation. Ankylosis should be recognized by the primary surgeon when palpating the ossicular chain to assess its mobility and usually occurs in the epitympanum.26 It is at least theoretically possible that ankylosis of the malleus or incus could occur after an initial surgery where these ossicles were found to be mobile. Etiologies for this acquired ankylosis include traumatic injury to the malleus or incus at the initial surgery and an intervening infection since the original surgery.27 Both of these scenarios are probably less likely than an unrecognized fixation of the ossicles that was present prior to the first surgery. Traumatic iatrogenic incus subluxation or complete dislocation could occur as a result of an inadvertent injury to the incus when operating in the middle ear. It could also occur after a purposeful maneuver at the first surgery, including palpation of the incus to assess its mobility, or at the time of prosthesis crimping. A perilymphatic fistula may be suspected in patients soon after their primary operation if fluctuating vertigo, dysequilibrium, sensorineural hearing loss, aural fullness, tinnitus, or sound distortion develops. Audiograms should corroborate the clinical complaint of fluctuations in hearing. The hearing loss is usually sensorineural. Cases of immediate sensorineural hearing loss are less likely to be successfully treated.25 In addition, patients who develop sensorineural hearing loss more than a year after stapes surgery that had used an oval window tissue seal should not be revised unless there is a history of trauma or dizziness.15 In cases with immediate or delayed sensorineural hearing loss without an oval window seal, findings of oval window fistulas are more common. Repair with a tissue seal may result in an improvement in dizziness and occasionally an improvement in hearing.25 Postoperative granulomas were more common in the era when Gelfoam was used to seal the oval window instead of a tissue seal. When granulomas occur, they occur most often in the first 8 weeks postoperatively.1 The symptoms are indistinguishable from a perilymphatic fistula with dysequilibrium, vertigo, and/or progressive sensorineural hearing loss. On physical examination, a red mass may be seen behind the tympanic membrane; however, the absence of this finding does not rule out the possibility of a granuloma being present. If a granuloma is suspected, high-dose steroids can minimize the inflammatory effect on the inner ear.1 It is thought that the granuloma is a foreign body reaction to Gelfoam, glove starch, Teflon fragments, and refractile particles in irrigation solution.26,28 The primary indications for revision stapedectomy are to restore a previously successful conductive hearing loss closure, to close a conductive hearing loss when an initial attempt has failed, to stabilize or possibly improve a sensorineural hearing loss due to a perilymphatic fistula or granuloma, and to improve vestibular symptoms due to these same two etiologies. Patients may also complain of dysacusis, diplacusis, and tinnitus. Part of the decision regarding a patient’s candidacy for revision stapes surgery is based on a review of the technique employed at the initial surgery and on the postoperative history after the primary stapes operation. An initial improvement of hearing with narrowing of the air–bone gap bodes well for a favorable result of a revision operation for a conductive hearing loss.25
Historical Overview
Meta-analysis of the Literature
Causes of Failure of Primary Surgery
Prosthesis-Related Failures
Ossicle-Related Failures
Incus Erosion and Necrosis
Malleus and Incus Fixation
Incus Subluxation
Footplate-Related Failures
Perilymphatic Fistula
Granuloma
Indications for Revision Surgery
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Revision Stapedectomy and Stapedotomy
