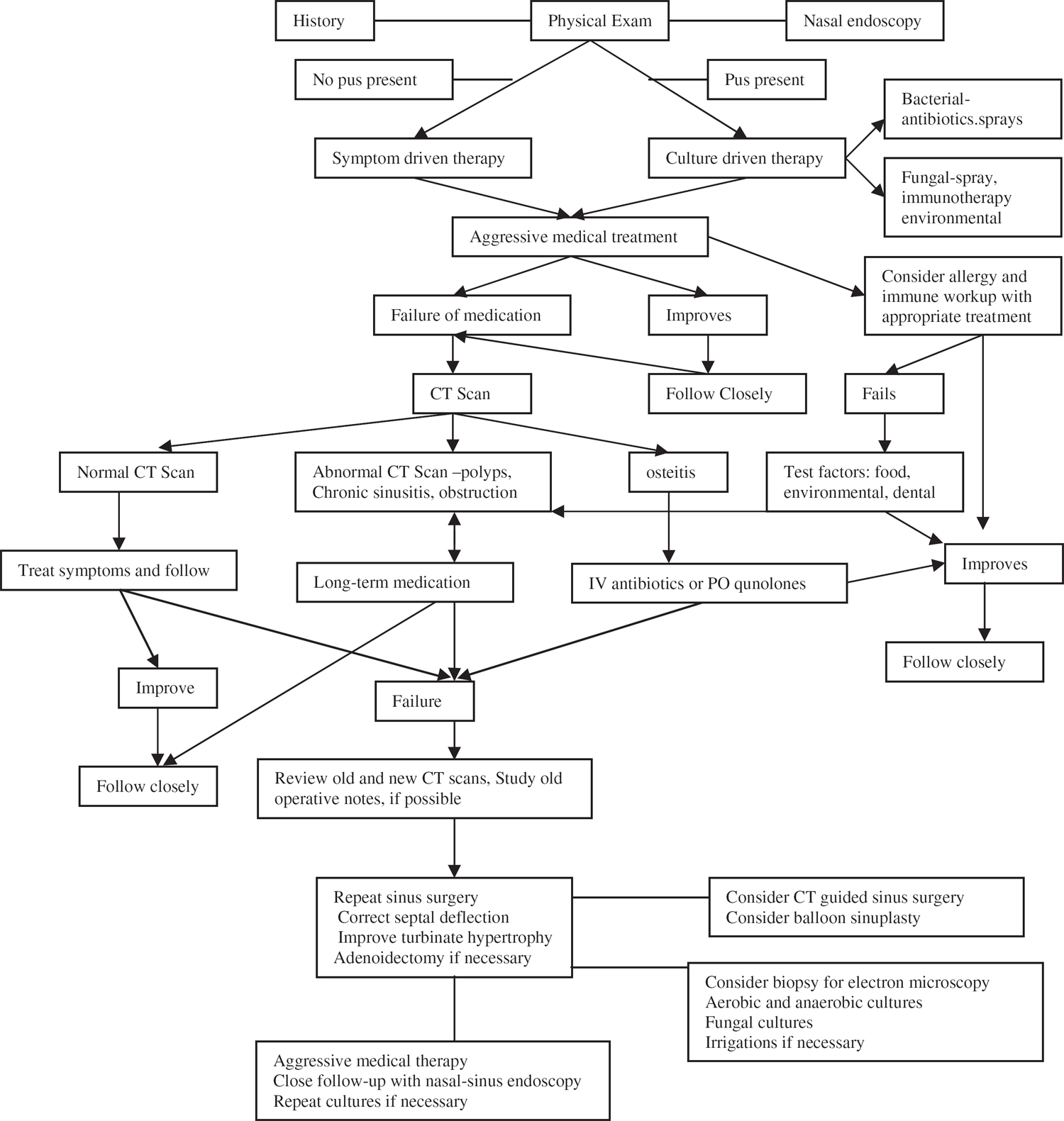
40 Revision Sinus Surgery of the Ethmoid Sinuses The effective, long-term treatment of patients with chronic rhinosinusitis represents one of the greatest challenges facing otolaryngologists. With chronic sinusitis becoming the leading chronic disease in the United States today, the issues associated with treating these patients have increased.1 Each patient with chronic sinusitis poses a very challenging quality of life issue for the physician.2,3 The improved effectiveness of diagnostic tools, such as rapid computed tomography (CT) scanning and endoscopic examination of the nose and paranasal sinuses, has led to more surgery. This rise in surgical volume, unfortunately, has also led to more failures, underscoring the need for doctors to understand both how to treat the long-term sinusitis sufferer and how to approach revision sinus surgery. The goal of any revision surgery should be to cure disease, to ameliorate symptoms, and to avoid complications. The significant failure rate experienced after initial sinus surgery is attributable to several different factors. First, sinusitis is not a monolithic disease but five different diseases grouped under one name. There is an anatomical form, an infectious form, an immunologic form, a ciliary dyskinesia form, and a mucus disorder form. Some forms of sinusitis are more amenable to effective cure by surgery than others. For example, the anatomical form of sinusitis, where there may be a septal deflection blocking the middle meatus outflow tract, is generally very curable through nasal and sinus surgery. However, most patients suffer from more than one type of this disease, leading to mixed surgical results. Second, the anatomy of the ethmoid sinuses makes them susceptible to initial surgical failures.4 Commonly called a labyrinth, the ethmoid sinuses are divided into three major sets of cells with several subsets and adjunctive cell groups. The ethmoids are made up of the infundibular cells, the bullar cells, and the posterior cells. Most ethmoid surgery involves the anterior two sets, the infundibular and the bullar cells, which drain through the middle meatus. Endoscopic sinus surgery drains these cells best through an anterior approach. A common source of surgical failure is the inability of many sinus surgeons to identify readily the middle and posterior drainage patterns through the superior meatus. The ground lamellar, which is the attachment of the middle turbinate to the lateral wall, may impede the drainage of bullar cells into the middle meatus. Thus, attention should be paid to opening the superior meatus, the “forgotten meatus.”5 Indeed, the sphenoethmoid recess is more important to the eventual success of severe ethmoid sinusitis cases than most surgeons realize. Although an anterior endoscopic approach to the posterior cells is possible, and makes it easy to visualize these cells postoperatively, they cannot drain unless they have easy dependent drainage, which is usually not possible to achieve through an anterior approach. Haller, Onodi, agger nasi, and sinus lateralis cells may also need to be identified preoperatively and intraoperatively to achieve full ethmoid sinus drainage. Finally, sinus surgery itself is not uniform. There are many variations in the types of sinus surgery performed depending on the physician’s background, training, philosophy toward the use of technology, and his or her perspective on miniature openings for sinus ostia.6,7 Depending on the approach taken in the initial procedure, the extent to which revision surgery may be required and its effectiveness can vary widely. For example, many patients who underwent sinus procedures before the advent of endoscopic sinus surgery had traditional inferior meatal openings, with the more natural middle meatal ostia being left untouched and blocked. Patients who underwent such Caldwell-Luc procedures without opening the middle meatus may now present with abnormal ciliary linings of the maxillary sinus due to the complete stripping of the natural respiratory mucosa, which was a common result of the older forms of maxillary surgery. Other patients may have had destructive middle turbinectomies as part of older intranasal sphenoethmoidectomies, which will reduce the effectiveness of the newer endoscopic approaches and thus limit long-term results. Some of these patients may have formed scarring or synechiae in the sinus outflow tracts, requiring wide débridements. Those patients who had only limited first-time surgery may need completion surgery. For example, some sinus surgeons choose to operate on only one side at a time, creating a need for revision surgery on the unoperated side. Other surgeons may have been loath to enter the frontal or sphenoid sinuses, leading to problems later on in the downstream ethmoid and maxillary sinuses. Finally, some surgeons never enter the more dangerous posterior ethmoid sinuses on the first surgery, hoping that the posterior cells will recover when the anterior ones clear. This variation in surgical approach makes evaluating the literature on failure rates somewhat difficult, given the need to understand authors’ experiences, philosophies, and approaches to first-time cases. Decision tree for chronic rhinosinusitis surgical failure Taking a complete history is one of the most important parts of the evaluation process for any revision ethmoid sinus surgery. It is vital for the surgeon to understand the patient’s history before the first procedure was performed to evaluate why the initial surgery did not succeed. The surgeon should inquire about such factors as prior medical and herbal therapies, antibiotics, sprays, allergy evaluation, and any other type of surgery. A full history may include information about, and tests of, the lower respiratory tract for asthma, pneumonia, and chronic bronchitis. This information may help point to causes of failure involving the mucosa or cilia. Allergies to aspirin and the presence of asthma can help in the diagnosis of Sampter syndrome, which has a very high recurrence rate. Prior sinus cultures may also be helpful to review. The presence of resistant staphylococcus and fungi may explain previous failure and help with postoperative planning if a second surgery is envisioned. It may be useful to ask for a computer printout from the patient’s pharmacist of all medications taken over the past year or so. Many patients forget the type, dosage, and order of medications taken. It is possible that a common medication has been overlooked, which could help the patient avoid revision surgery or help improve the results of such surgery. It is very important to review the records, including previous operative reports, of any other surgeon who has operated on the patient to have a road map of the success or failure of previous treatments. Before planning revision surgery, the conditions of areas such as the septum, middle turbinates, sinus meati, and special ethmoid cells should be carefully evaluated. Any complications to the fovea ethmoidalis or lamina papyracea as well as bleeding should be highlighted and identified. The patency of the sphenoid ostia and the frontal duct also should be investigated in the operative reports.8 Unfortunately, operative dictations are not always complete or mention all areas of interest. Many surgeons, for example, do not note thinning of the lamina or report every breach of the orbit, even though they should. Young sinus surgeons should be trained to spend time on their dictations and to develop a consistent style of reporting indications, findings, and surgical approaches accurately. Even if an area is not touched, for example, it should be mentioned in the operative report both to help with postoperative care and to record the fact that the surgeon thought about the possibility of unrecognized disease in that area. Every residency training program should periodically read, review, and grade the accuracy and reliability of surgical dictations to instill an understanding of the important role that accurate documentation plays in patient care (and surgical billing). A fine-cut CT scan with 1 mm cuts is an essential element in the work-up of sinus surgical failures. The surgeon should ask for axial, coronal, and sagittal views, if available. Axial views provide an anteroposterior dimension. They can help the surgeon find the lateral wall of the posteriormost ethmoid cells and the sphenoid cells by helping to determine whether the lamina papyracea is flat or triangular in relationship to the orbital apex.9 Coronal views help illuminate the ostiomeatal complex and the differences between the two sides. A coronal view can also help to identify higher cells on one side that may have been unopened during the first sinus surgery. This view will be essential if the frontoethmoid recess is to be opened at the time of revision surgery. Both axial and coronal views may help to identify areas of possible osteitis, particularly of the sphenoid sinus and orbital apex. Patients with suspected osteitis should be treated with either a course of long-term quinolone antibiotics or intravenous (IV) antibiotics prior to surgery.10 The sagittal view is underappreciated for its ability to help identify the drainage patterns of the posterior sinuses. In particular, sagittal views can aid the surgeon in determining the position of the ground lamella, which gives the insertion of the middle turbinate into the lateral wall. The superior meatus may lie anterior to the ground lamella or above it. Polyps growing from the posterior ethmoid sinuses may be appreciated blocking the superior meatus and only be identifiable on the sagittal views. To avoid complications of surgery in scarred bullar cells, it is essential to determine the position of the base of the skull and the down sloping of the middle ethmoid cells. Sagittal views also help to orient the revision sinus surgeon as to the dangerous angles and location of any infected cells at the base of the skull. Comparing a current CT scan with a CT scan taken before the first surgery can also be helpful if the original preoperative scan is available. Such a comparison may help to differentiate between retained cells, scarring from the first surgery, and problem areas. A comparison of the two CT scans, for instance, can identify new areas of infection and areas of sinusitis inadvertently caused by the first surgery. It is essential to identify these areas to avoid making the same mistakes twice. Additionally, this comparison may highlight small but important deflections of the septum and floppy middle turbinates. One of the classic mistakes made by inexperienced surgeons is to send a patient for a CT scan at an inopportune time. CT scanning should only be performed after maximal medical therapy, including antibiotics and topical steroid nasal sprays. The antibiotic course should be individualized from 10 days to 3 weeks, depending on the patient’s problem and prior therapies. Allergy care should be included in the presence of immune or allergic disease. Another common mistake some physicians make is to have CT scans taken before the nose and sinuses have had a chance to heal completely after the initial sinus surgery. It may take more than 12 weeks for the mucosa of the sinuses to calm down. During this period, any scarring and mucosal disease should be treated by medication, such as steroids, or by office endoscopic manipulation in mini “touch-up” procedures. Performing a CT scan too soon after surgery may overemphasize recurrence and recidivism. CT scanning should be ordered by the rhinologist and not by an internist or family practitioner, who may not fully understand the timing or postoperative care issues. If possible, the same radiologist should be asked to compare the two CT scans. Earlier CT scanning should be performed only if there are any complications, such as visual disturbances or a suspected cerebrospinal fluid (CSF) leakage. Serial CT scanning is usually unnecessary, as a complete sinus procedure should provide ample exposure to the relevant sinuses by the use of rigid or flexible endoscopes. A magnetic resonance imaging (MRI) scan has limited efficacy in identifying sinus surgery failures. Many patients with headaches are sent for MRIs, which can overstate the inflammation present in the nose and paranasal sinuses, particularly on T2-weighted images. Edematous mucosa and submucosa are hyperintense on T2-weighted images. After administration of gadolinium, the mucosa may enhance even more. Although retained secretions do not enhance on T1-weighted images after gadolinium, in chronically obstructed sinuses, the water may be absorbed and more proteinaceous, thereby appearing more intense on T1-weighted images. Patients are often told that they have recurrences following an evaluation of an MRI, when all that they truly have is viral inflammation or allergic mucosal disease. An MRI may be helpful, however, in identifying an encephalocele or a meningoencephalocele. Orbital problems may be further highlighted through an MRI if there is possible disease in the orbital apex. Fat suppression techniques, for instance, may help the radiologist and surgeon differentiate between normal fat and an orbital abscess. An MRI may also be helpful in identifying the posterior extent of the frontal sinus, although it is of only limited use in outlining the essential ostiomeatal complex. Finally, an MRI and MR angiogram of the sphenoid may help to differentiate mucosal disease from the carotid artery in revision cases. When examining a possible candidate for revision surgery, special attention should be paid to the nasal septum, the turbinates, the two major meati, the sphenoethmoid recess, the nasopharynx, the larynx, and the trachea. During the physical examination of the nose, measurements and angles may be taken to the base of the skull on both sides and to the face of the sphenoid. Although the use of CT-guided surgical techniques may make these measurements seem obsolete, this approach to the sinuses still helps to focus the surgeon’s attention on the differences between, and problems individual to, each side of the nose. The angles required for introduction of the endoscope should be recorded to avoid anterior penetration of the skull base during surgery. Endoscopic identification of the lamina papyracea and of any related scars blocking its easy examination may help to pinpoint areas of recurrent disease and danger to the orbit. In addition, documenting the patient’s gross visual acuity and extraocular movements may be helpful if there is any risk to the orbits or a prior history of diplopia or diminished visual acuity.
Evaluation for Revision Cases
History
CT and MRI Evaluation
Focused Examination
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


