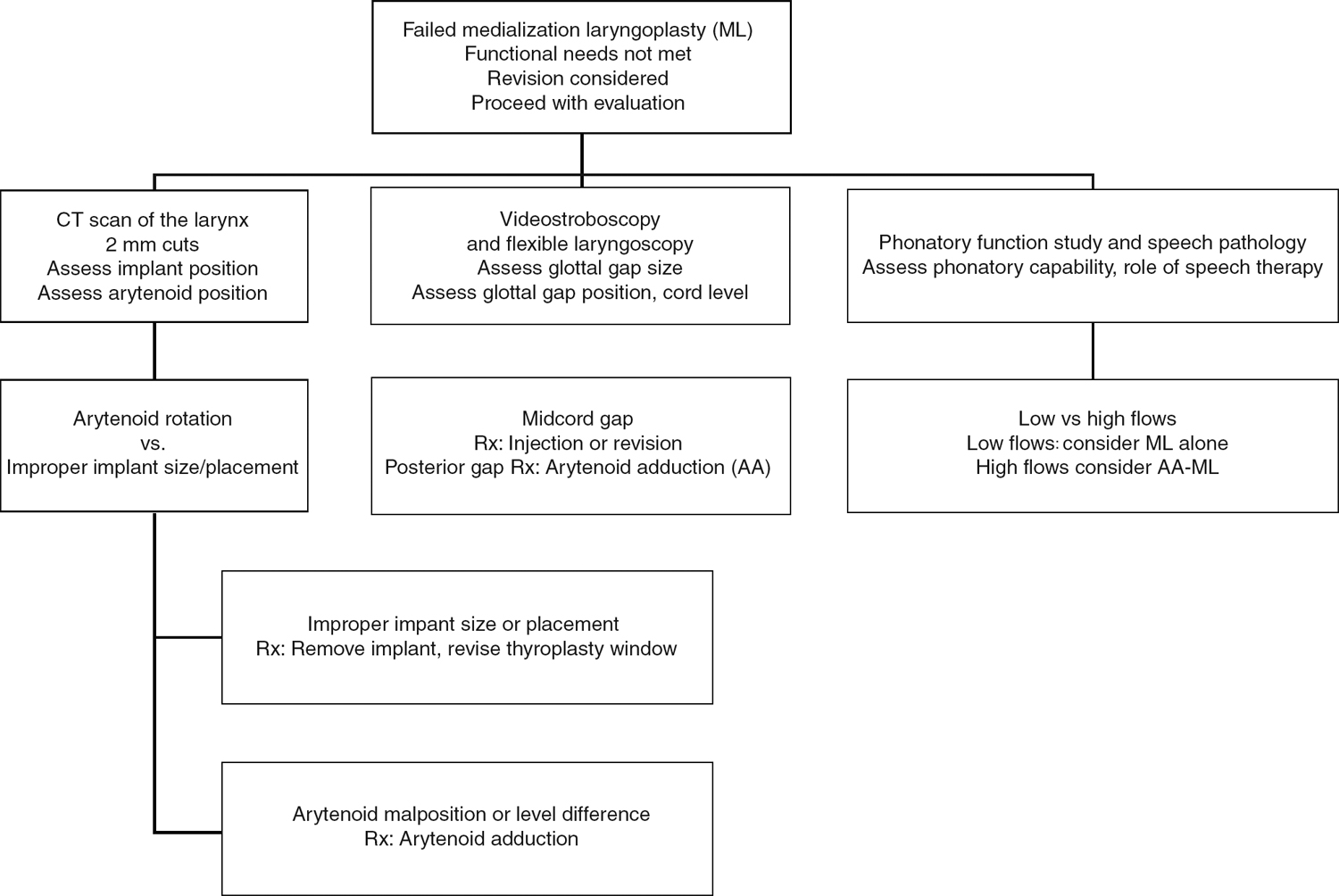
4 Revision Medialization Laryngoplasty The concept of medialization laryngoplasty has been with us since the turn of the last century. Payr in 1915 first described medialization laryngoplasty using an anterior pedicled U-flap on the thyroid cartilage.1 Seiffert and Meurman described the implantation of a rib cartilage into the paraglottic space to medialize the vocal folds.2,3 However, the laryngeal framework fell into disfavor because of airway compromise, postoperative infections, and the introduction of injection laryngoplasty. In 1911, Brünnings successfully reported the use of intracordal paraffin injections to medialize vocal folds in glottic insufficiency.4 This method fell into disrepute because patients developed complications such as paraffinomas and distal spread of paraffin. Arnold, in 1962, described the use of Teflon (polytetrafluoroethylene), which is still used today but is gradually diminishing in popularity because of the numerous complications associated with its use.5–7 Other materials, such as collagen and autologous fat, have come to the forefront and are popularly used today.8,9 It was not until 1974, when Isshiki et al described a systematic approach to surgery of the vocal skeleton to change the tension and mass of the vocal fold, enabling many surgeons to similarly achieve good results, did laryngeal framework surgery become popular.10 They described four different types of laryngeal framework surgery for different clinical conditions. Type 1 thyroplasty (medialization laryngoplasty) is the most popular method of laryngeal framework surgery because it addresses the most common clinical disorder of glottic incompetence caused by vocal fold paralysis.11 Medialization laryngoplasty reduces glottic incompetence and helps prevent aspiration. Glottic incompetence may arise from 1. Paralysis of the vagus nerve 2. Vocal fold atrophy (e.g., presbyphonia) 3. Sulcus vocalis When the vagus nerve is damaged, the vocal fold may assume one of three positions: median, paramedian, or lateral. In patients with a unilateral vocal fold paralysis with the vocal fold in the paramedian or lateral position, the uninvolved side often compensates for a glottic gap by coming across to meet the paralyzed side, thereby resulting in a good or satisfactory voice. However, there are instances when this compensatory mechanism is insufficient and will result in a patient who is dysphonic and breathy. Often the patient then acquires undesirable compensatory measures, such as excessive laryngeal squeezing or laryngeal muscle tension, resulting in a strained, effortful voice. At this point, the patient often presents to the clinic requesting professional help. Medialization laryngoplasty aims to restore vocal strength, loudness, sustainability, and projection. In high vagal lesions, there may be paresthesia or hypoesthesia of the supraglottis, resulting in laryngeal penetration and aspiration. Medialization thyroplasty has been shown to help reduce aspiration in these patients. Medialization laryngoplasty can be divided into 1. Injection laryngoplasty 2. Laryngeal framework surgery a. Vocal fold medialization b. Arytenoid adduction c. Cricothyroid approximation Injection laryngoplasty improves the voice quality by injecting a material into the vocal fold. Materials may be injected medially into the superficial lamina propria (e.g., vocal fold scarring) or laterally in the vocal ligament or vocalis muscle. Superficial injection techniques aim to re-create the superficial layer of the vocal fold in an attempt to re-create the mucosal wave. Lateral or deep injections attempt to augment the vocal fold by adding bulk and improving glottic closure. This lateral injection is most useful in treating vocal fold paresis, paralysis, and vocal fold atrophy. Over the last 2 decades, many different materials have been tried and tested. The choice of material depends on patient factors, safety profile of the material, resorption characteristics, and the surgeon’s experience with the material. Fat, micronized dermis, collagen, Gelfoam, and hydroxylapatite are some of the materials being used today.8,9,12,13 Decision tree for evaluation of failed medialization laryngoplasty The advantages of injection laryngoplasty are as follows: 1. It is easily performed. 2. It is quick and effective. 3. It is convenient, for both the patient and the surgeon, if performed using indirect laryngoscopy transorally under local anesthesia or transcutaneously as an office procedure. There are also several disadvantages: 1. The anatomy of the vocal fold and arytenoid cartilage is altered in paralysis. The arytenoid is tilted anteriorly and rotated laterally. There is a vertical phase difference between the two vocal folds. Injection laryngoplasty does not address these issues. 2. The diffusion pattern of the substances injected follows the path of least resistance and may not adequately augment the areas intended. 3. Although the substances are biologically inert and are generally well accepted by the body, hypersensitive and inflammatory reactions can occur, resulting in granuloma formation and vocal fold scarring. 4. These substances may interfere with the mass, volume, and pliability of the vocal fold. 5. These procedures are irreversible and difficult to correct. 6. Several repeated procedures may be required because of absorption. 7. If performed under general anesthesia, voice monitoring is not possible. If performed under local anesthesia, the procedure may be technically demanding, as patient cooperation is required. Isshiki et al described four types of laryngeal framework surgery.15 Type 1 thyroplasty medializes the vocal fold by insinuating an implant between the thyroid cartilage and the thyroarytenoid muscle, thus medializing the vocal fold. This is the most popular thyroplasty procedure, and it addresses the glottic insufficiency resulting from vocal fold paresis or paralysis. It may be supplemented with arytenoid adduction when there is a large posterior glottic gap that cannot be corrected by medialization alone.16 Type 2 thyroplasty lateralizes a segment of the thyroid cartilage, thus lateralizing the vocal fold. It increases the glottic chink, resulting in a breathy voice. It was first proposed as an alternate treatment for adductor spasmodic dysphonia. Type 3 thyroplasty shortens the anteroposterior distance, resulting in a lax vocal fold and pitch lowering. It is used in the treatment of therapy-resistant mutational dysphonia and vocal fold atrophy. Type 4 thyroplasty increases the anteroposterior dimensions of the thyroid ala, thus thinning out the vocal folds with consequent increase in pitch. This is appropriate for patients undergoing gender reassignment or those with cricothyroid muscle paralysis. Medialization laryngoplasty can be unilateral or bilateral. Bilateral medialization is indicated for patients with presbylaryngis, unilateral paralysis with contralateral vocal fold bowing/atrophy, bilateral vocal fold paresis, and recalcitrant abductor spasmodic dysphonia. In addition, two other procedures can be performed with medialization laryngoplasty: arytenoid adduction or arytenoidopexy cricothyroid approximation and subluxation. The classical arytenoid adduction procedure described by Isshiki et al achieves rotation of the arytenoid by suture placed through the muscular process.15 The suture is directed anteriorly through the thyroid lamina, thus mimicking the lateral cricoarytenoid muscle and the thyroarytenoid muscles. The arytenoidopexy technique described by Zeitels simulates the agonist-antagonist adductor function of the other intrinsic muscles (lateral thyroarytenoid, interarytenoid, posterior cricoarytenoid) as well.17 Zeitels showed it to be more effective than the classic arytenoid adduction in closing interarytenoid gaps through cadaveric studies. Cricothyroid approximation mimics the function of the cricothyroid muscle in lengthening the vocal folds. In vocal fold paralysis, there may be anterior tilting of the arytenoids cartilage, leading to a vertical phase height difference. The denervated vocal fold also undergoes atrophy and becomes flaccid. Some surgeons will perform routine manual cricothyroid approximation intraoperatively to see if correcting the vocal fold tension will further improve the voice. Criocothyroid subluxation was described by Zeitels to complement his arytenoidopexy technique because of the disruption to the cricothyroid joint during the procedure.17 This caused the thyroid lamina to be retrodisplaced with relation to the cricoid, resulting in a foreshortened vocal fold. Zeitels also found that cricothyroid subluxation improved the aerodynamic efficiency of the glottal valve, leading to better acoustic maximal-range capabilities. Complications of medialization laryngoplasty have been reviewed by Tucker and by Rosen.18,19 These include immediate and delayed complications. Immediate complications include airway edema, stridor, and bleeding. Delayed complications include poor voice outcome, implant extrusion, dysphagia, and airway obstruction. The impact of physician experience, selection of the implant, and medialization laryngoplasty versus medialization with arytenoid adduction all have an impact on outcome. For the patient with poor voice or airway outcome after prior medialization laryngoplasty, revision surgery may be necessary. Revision surgery may be accomplished by simple injection laryngoplasty to major revision, such as revision medialization with arytenoid adduction.20 Careful assessment and analysis should reveal the deficit that needs further correction in these patients. After a complete analysis, revision surgery based on surgery designed to correct the deficit will often offer an improvement in the functional capacity of the patient. A general systemic and comprehensive voice evaluation is performed. A detailed history into the symptoms and duration of disability is taken. The specific vocal needs and outcome expectations are discussed, and treatment is recommended. An extensive evaluation, including a thorough examination of the head, neck, and chest region, is performed to exclude an obvious cause of the vocal fold paralysis. Computed tomography (CT) scans assist in evaluating the entire course of the vagus nerve. In the patient with prior surgery, a CT scan of the larynx done without contrast at 2 mm intervals is recommended. The CT scan serves the following functions: (1) it delineates the position of the implant and the site of medialization, (2) it will show the position of the arytenoid cartilage on the paralyzed side relative to the normal side, (3) it will show whether there is adequate soft tissue coverage of the implant and will show an impending extrusion, (4) it will demonstrate the position of the previous thyroplasty window, and (5) it will demonstrate the level differences between the vocal folds.
Indications and Contraindications
Treatment
Nonsurgical Treatment
Materials
 Teflon: Teflon is a polymer of polytetrafluoroethylene. After injection into the paraglottic space, an acute inflammatory reaction ensues that later becomes chronic and encapsulates the polymer. Although good results are achieved immediately, the long-term results are more difficult to predict and may deteriorate over time. Another problem associated with Teflon use is migration superficially within the vocal fold, eroding the overlying mucosa and leading to granuloma formation. This affects the mucosal wave adversely and causes stiffness. Local spread to lymph nodes and the thyroid gland has been described.7 The current indication for Teflon injection is for patients with vocal fold paresis or paralysis with terminal disease and short life expectation.
Teflon: Teflon is a polymer of polytetrafluoroethylene. After injection into the paraglottic space, an acute inflammatory reaction ensues that later becomes chronic and encapsulates the polymer. Although good results are achieved immediately, the long-term results are more difficult to predict and may deteriorate over time. Another problem associated with Teflon use is migration superficially within the vocal fold, eroding the overlying mucosa and leading to granuloma formation. This affects the mucosal wave adversely and causes stiffness. Local spread to lymph nodes and the thyroid gland has been described.7 The current indication for Teflon injection is for patients with vocal fold paresis or paralysis with terminal disease and short life expectation.
 Gelfoam: Gelfoam, which is supplied as a powder and mixed with a buffered saline solution to form a paste, is used for vocal fold injection. Because it lasts only 6 to 8 weeks, it is ideal for temporary treatment for vocal fold paralysis when recovery is expected. It can also be used repeatedly in the first few months before recovery when vocal fold function is essential.
Gelfoam: Gelfoam, which is supplied as a powder and mixed with a buffered saline solution to form a paste, is used for vocal fold injection. Because it lasts only 6 to 8 weeks, it is ideal for temporary treatment for vocal fold paralysis when recovery is expected. It can also be used repeatedly in the first few months before recovery when vocal fold function is essential.
 Fat: Autologous fat is readily harvested and available. It does not give a foreign body reaction and is well tolerated. There are different methods of harvesting fat. Some surgeons prefer harvesting abdominal fat with a liposuction machine, whereas others prefer careful dissection with minimal trauma to maintain integrity of the lipocytes. The harvested fat is processed and loaded into a Brünings syringe for injection. The author washes the fat in Ringer’s lactate solution followed by Depo-Medrole steroid solution before loading it into a syringe. Other authors prefer centrifuging the fat to remove impurities. Approximately 30 to 50% of injected material will reabsorb within the first month; hence it is advisable to overcorrect when performing lipo-injection. Fat is injected lateral to the vocal folds in vocal fold paralysis.
Fat: Autologous fat is readily harvested and available. It does not give a foreign body reaction and is well tolerated. There are different methods of harvesting fat. Some surgeons prefer harvesting abdominal fat with a liposuction machine, whereas others prefer careful dissection with minimal trauma to maintain integrity of the lipocytes. The harvested fat is processed and loaded into a Brünings syringe for injection. The author washes the fat in Ringer’s lactate solution followed by Depo-Medrole steroid solution before loading it into a syringe. Other authors prefer centrifuging the fat to remove impurities. Approximately 30 to 50% of injected material will reabsorb within the first month; hence it is advisable to overcorrect when performing lipo-injection. Fat is injected lateral to the vocal folds in vocal fold paralysis.
 Collagen: The use of collagen was popularized by Ford et al in the human larynx.8 Safety issues with bovine collagen, such as hypersensitivity reactions, have led to the introduction of autologous human collagen for injection laryngoplasty. Although collagen is absorbed by the body, the amount and rate of it are less than those of fat.
Collagen: The use of collagen was popularized by Ford et al in the human larynx.8 Safety issues with bovine collagen, such as hypersensitivity reactions, have led to the introduction of autologous human collagen for injection laryngoplasty. Although collagen is absorbed by the body, the amount and rate of it are less than those of fat.
 Other materials: Materials such as autologous fascia harvested from the fascia lata have been reported with good success in a small series.14 The rate of resorption is low, and the free grafts survive as living tissue. Micronized dermis is an off-the-shelf product that is reconstituted by the surgeon and is well tolerated. The material does not require hypersensitivity testing and may be given as an office procedure, as there is no donor morbidity. Absorption is still high, and overinjection by 50% is necessary.12
Other materials: Materials such as autologous fascia harvested from the fascia lata have been reported with good success in a small series.14 The rate of resorption is low, and the free grafts survive as living tissue. Micronized dermis is an off-the-shelf product that is reconstituted by the surgeon and is well tolerated. The material does not require hypersensitivity testing and may be given as an office procedure, as there is no donor morbidity. Absorption is still high, and overinjection by 50% is necessary.12
Advantages and Disadvantages
Surgical Treatment
Preoperative Evaluation
History
Examination
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Revision Medialization Laryngoplasty
