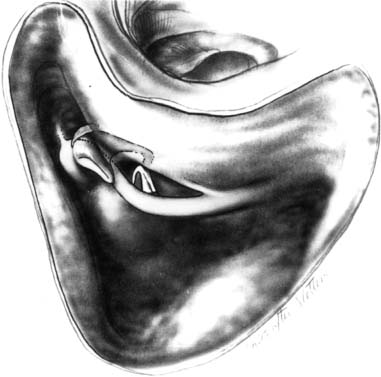
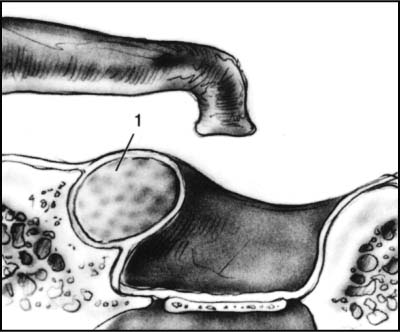
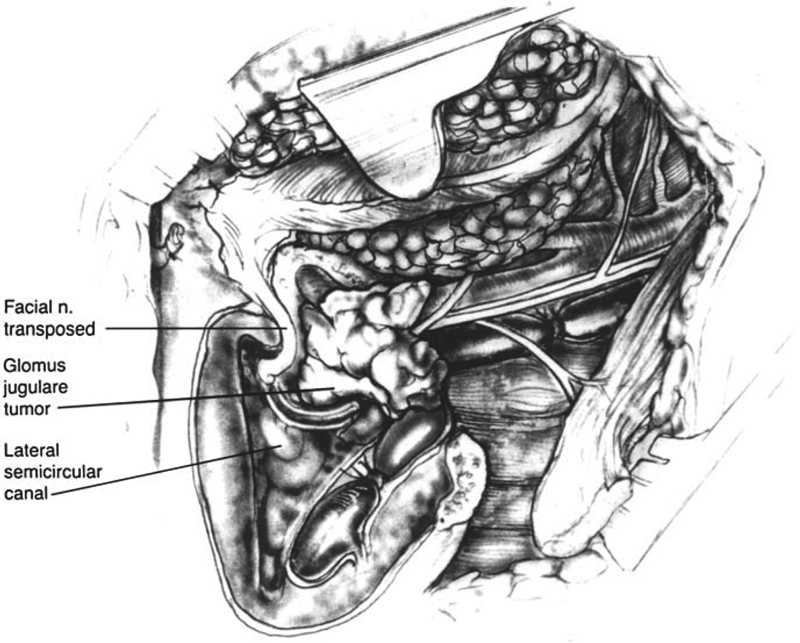
14 Revision Facial Nerve Surgery Most revision otologic and neuro-otologic surgery requires some attention to the facial nerve. Revision surgery on and around the facial nerve is particularly challenging because the landmarks that guide the surgeon to the location of the facial nerve in primary surgery have often been altered or are completely absent in the revision case. This may be compounded by fibrosis, scar, or the recurrence of disease closer to the nerve than before. Surgeons experienced with revision surgery involving the facial nerve are aware of these difficulties, so in primary procedures where revision may be a possibility at some later time, all attempts are made to preserve the normal architecture. An essential requirement to perform revision surgery and avoid injury to the facial nerve is a thorough knowledge of temporal bone anatomy at those landmarks, which can be used to pinpoint the location of the facial nerve. Continuous electromyography (EMG) facial nerve monitoring is a valuable adjunct in this difficult surgery. The seventh cranial nerve (CN VII) exits the brainstem at the pontomedullary groove medial to the root entry zone of the vestibulo-cochlear nerve. It joins the nervus inter-medius and eighth cranial nerve (CN VIII) traveling through the pontine cistern before passing into the porus of the internal auditory canal. A loop of the anteroinferior cerebellar artery (AICA) often passes into the medial portion of the internal auditory canal, where it gives off the labyrinthine artery to the inner ear. In this region the loop of the AICA may lie in the plane between the facial nerve anteriorly and the vestibular nerve posteriorly. The facial nerve then courses in the anterosuperior position of the internal auditory canal to pass above the transverse crest and anterior to Bill’s bar before passing through the meatal foramen at the lateral end of the internal auditory canal. At the meatal foramen, the dura continues as the epineurial sheath of the facial nerve and contains portions of the arterial supply, including branches of the superior petrosal artery from the AICA and the stylomastoid artery, a branch of the postauricular artery supplying the distal portion of the nerve. In addition, venous plexuses are found within the epineurium. The intracranial portion, in contrast, lacks an epineurium and is therefore less resistant to mechanical manipulation. The labyrinthine portion distal to the meatal foramen courses over the cochlea to the geniculate ganglion, where it gives off the greater superficial petrosal nerve, which carries parasympathetic secretomotor fibers ultimately destined for the lacrimal gland. The facial nerve then turns posteriorly and courses along the medial wall of the middle ear, passing superior to the cochleariform process and over the superior margin of the oval window. Dehiscence of the bony canal has a reported incidence of up to 50%, with the most common area of dehiscence being located over the oval window.1 The nerve then turns inferiorly, passing inferior and medial to the lateral semicircular canal to run down to the stylomastoid foramen. In this vertical segment it gives off (in order from superior to inferior) the motor branch to the stapedius muscle, a sensory branch to the skin of the external auditory canal, and the chorda tympani nerve. Upon exiting from the temporal bone through the stylomastoid foramen, it gives off motor branches to the auricularis posterior muscle and the posterior belly of the digastric muscle. It then passes into the substance of the parotid gland, where it divides into three upper divisions and two lower divisions to form the pes anserinus. Currently, facial nerve monitoring is used commonly when the surgical dissection directly involves the facial nerve, or when the nerve is at risk because of unusual location or other factors. There is no consensus regarding its role in revision middle ear or mastoid surgery,2 nor are there any data supporting its efficacy in these situations. EMG-based facial nerve monitoring offers crucial scrutiny when compared with sonar-based systems. Some experts advocate use of facial nerve monitoring in revision middle ear and mastoid surgery when there were problems with the facial nerve at the initial surgery, such as a postoperative paralysis. During revision of these cases, care should be taken to avoid inadvertently anesthetizing the facial nerve with injections of lidocaine and epinephrine, which would not only render the facial nerve monitoring useless, but turn it into a liability and potentially put the facial nerve at higher risk for injury. In revision cases requiring external auditory canal injections or cases where there is a mastoid cavity, we use injections of epinephrine diluted to 1:100,000 without lidocaine for hemostasis. This avoids the problem of inadvertent anesthesia to the facial nerve. If facial nerve monitoring is to be used in a patient with a preoperative partial facial weakness, one must place the monitoring electrodes in areas of the face with the maximal amounts of facial nerve movement. In these cases, higher than usual levels of current may be required when stimulating the nerve. Lastly, it cannot be overstressed that the anesthetic staff understand that a facial nerve monitor is being used and that they avoid the use of paralyzing drugs, except for a short activity agent at the time of induction of anesthesia. In revision mastoid surgery for chronic otitis media, pre-operative computed tomography (CT) scanning to identify the facial nerve may not be very helpful, because the soft tissue that is invariably present can make it difficult to determine if the facial nerve is dehiscent. Recurrent or residual cholesteatoma in a previous intact canal wall mastoidectomy is not unusual and may be removed at the planned second stage (12 months after the primary surgery) via the tympanotomy and facial recess. Although the facial nerve is usually at risk in the area of the facial recess and epitympanum (Fig. 14.1), the tympanic segment of the facial nerve has the highest incidence of iatrogenic facial nerve injury during mastoid surgery.3 Areas of dehiscence created by either the disease process (cholesteatoma) or the surgery should be noted at the primary procedure so that care may be taken in those areas at the second stage or during revision surgery. Risk to the facial nerve is more significant when revising a canal wall down mastoidectomy. For example, canal incisions should be made lateral to the location of the facial nerve to avoid injury. To achieve this, the bulge of the lateral semicircular canal should be used as a guide to the location of the facial nerve and the incisions made posterior and to this region. The tympanomeatal flap should be elevated carefully over the lateral semicircular canal and forward over the facial ridge. Initial elevation of the flap over the inferior aspect of the facial ridge generally avoids the facial nerve, as the residual bone is usually thicker at that point. The bone over the facial nerve should be palpated with a blunt instrument, such as a gimmick elevator or the side of a sickle knife. Skin over a dehiscent facial nerve should readily dissect away from the sheath of the nerve unless the sheath and/or nerve had been injured during the previous surgery. In this situation a facial nerve monitor and stimulating probe are very useful to aid identification of the nerve. Once the middle ear cleft is entered, secondary landmarks, such as the oval window (immediately inferior to the facial nerve) and cochleariform process (immediately inferior and anterior to the facial nerve), are used to pinpoint the course of the facial nerve. Once the course of the nerve is appreciated, the recidivistic cholesteatoma can be safely removed. Fig. 14.1 The course of the facial nerve is depicted for a right canal wall up mastoidectomy with the facial recess open. Recurrent cholesteatoma involving the mastoid tends to occur in areas of the facial recess and epitympanum and therefore adjacent to the facial nerve through its course in these areas. (From Brackmann DE, Shelton C, Arriaga MA, eds. Otologic Surgery. Philadelphia: WB Saunders; 2001. Reprinted with permission.) The facial nerve may be vulnerable during revision stapedectomy or ossiculoplasty surgery if dehiscent and/or prolapsed over the oval window. It is important to recognize early in the operation if the facial nerve is dehiscent. This can be determined by palpation (Fig. 14.2). Facial nerve identification can be difficult in revision cases due to the distortion of the anatomy by fibrous tissue. The cochleariform process is a useful landmark to locate the anterosuperior aspect of the oval window. The facial nerve will be directly superior and posterior to the cochleariform process. Initial identification of the inferior margin of the oval window can allow for its identification in a circumferential fashion, which will also allow identification of the facial nerve. Particularly in revision stapedectomy surgery, adequate removal of the bone of the scutum will permit adequate visualization of the anatomy in this area. Fig. 14.2 Dehiscent facial nerve shown overhanging the oval window. In this situation, identification of the facial nerve is important, but it is generally possible to work past it to complete the operation. (From Brackmann DE, Shelton C, Arriaga MA, eds. Otologic Surgery. Philadelphia: WB Saunders; 2001. Reprinted with permission.) Before using a laser in the oval window, it is important to determine whether it is dehiscent and what its location is in relationship to the previously placed prosthesis. Laser facial nerve injury is very rare, but it is a potential pitfall best avoided. Revision surgery for glomus tumors is particularly difficult when an infratemporal fossa approach was used during the primary surgery, as this involves closure of the ear canal and transposition of the facial nerve. Furthermore, the facial nerve may be surrounded by a fat graft. After making skin incisions, the surgeon should try to identify the margins of the bony defect. The mastoid tip is absent, as it is typically removed during the initial procedure. The superior bony margin is usually intact, and one can follow it forward to the root of the zygoma and temporomandibular joint. With these landmarks, the middle fossa dural plate (or dura) is traced medially. Once the labyrinth is identified, the facial nerve can be found just superior to the cochleariform process (Fig. 14.3). The nerve is typically in the normal anatomical position in this area, and may also be found in the remnant of the fallopian canal in its horizontal portion, if it was replaced in that location at the previous procedure. The facial nerve usually separates from the surrounding fat graft and can be verified using the facial nerve monitor. Inferior to the mastoid genu, there is no bony support for the nerve, and it tends to be surrounded by fat and fibrous tissue. It is necessary to mobilize the facial nerve enough to transpose it anteriorly, but it does not have to be skeletonized, and some fat and fibrous tissue can be left attached, as long as its bulk does not impede visualization. Fig. 14.3 Infratemporal fossa approach for a right ear. Note the bony margin of the mastoid cavity superiorly along the middle fossa dural plate. The facial nerve is shown transposed, but it remains in the normal anatomical position adjacent to the cochleariform process and can be identified in this area. (From Brackmann DE, Shelton C, Arriaga MA, eds. Otologic Surgery. Philadelphia: WB Saunders; 2001. Reprinted with permission.) Recurrence of glomus tympanicum tumors is typically related to inadequate exposure during an initial transcanal removal. Removal of these tumors through an extended facial recess approach usually provides the adequate access.4 Recurrent acoustic tumors are uncommon, with the majority reported after initial retrosigmoid removal.5 Residual tumor left behind in the internal auditory canal is generally felt to be responsible for these recurrences.6 Tumor recurrence after initial complete translabyrinthine removal is very rare and occurs in less than 1% of cases.7,8 After middle fossa removal, there have only been scattered reports of recurrences identified. For removal of recurrent acoustic tumors, we prefer the translabyrinthine approach, as it provides positive intratemporal facial nerve identification in a location not involved with previous scar tissue and with very predictable anatomy. Scar tissue in the posterior fossa can obscure the proximal facial nerve location and make its identification more difficult. Facial nerve monitoring is very helpful in these cases as well. The facial nerve is identified laterally at Bill’s bar (Fig. 14.4
Review of the Anatomy of the Facial Nerve
Facial Nerve Monitoring
Revision Surgeries in which the Facial Nerve May Be at Risk
Mastoid Surgery for Chronic Otitis Media
Middle Ear Surgery
Glomus Tumors
Acoustic Tumors
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


