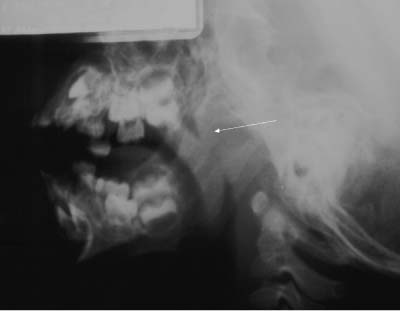
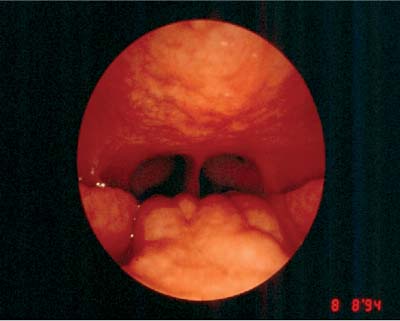
45 Revision Adenotonsillectomy The need for revision adenotonsillectomy is not common, but it does occur on occasion. The failure of initial surgery may be related to patient or physician factors. To understand the regrowth of adenoids or tonsils, a comprehensive understanding of the anatomy of the nasopharynx, oropharynx, and Waldeyer ring, as well as the disease processes and surgical techniques, is required. Sometimes the recurrence of symptoms does not correlate with adenotonsillar hypertrophy. The nasopharynx lies between the soft palate and the nasal choanae and communicates with the nasal cavities, eustachian tube, and oropharynx. The boundaries of the nasopharynx are the free edge of the soft palate anteriorly, posteriorly by the pharyngeal wall, and laterally by the palatopharyngeal arches. In the newborn, the nasopharynx is short and follows a gentle curve (small anteroposterior diameter), whereas the nasopharynx and oropharynx form an angle of almost 90 degrees by puberty. The adenoids are located in the roof of the nasopharynx at the skull base. The oropharynx is the posterior continuation of the oral cavity beyond the tonsillar pillars. The anterior palatine pillar is formed by the palatoglossus muscles, the posterior palatine pillar by the palatopharyngeus muscles. Between the two arches are the palatine tonsils. At birth, the base of the tongue and the larynx are high in the neck, with the epiglottis overlapping the soft palate. The base of the tongue and the larynx descend with growth and reach the adult location by age 4, when the base of the tongue and the lingual tonsils form a part of the anteroinferior wall of the oropharynx. The oropharynx is lined with stratified squamous epithelium. The lamina propria contains connective tissue, seromucinous glands, and numerous neutrophils, lymphocytes, and plasma cells. A ring of lymphoid tissue, called the Waldeyer ring, encircles the proximal end of the aerodigestive tract. This structure is comprised of three major lymphoid aggregates (pharyngeal tonsils and adenoids, palatine tonsils, and lingual tonsils) and four minor lymphoid aggregates (tubal tonsils, lateral pharyngeal bands, pharyngeal granulations, and lymphoid tissue in the laryngeal ventricle). The pharyngeal tonsil tissue (adenoids) is located in the roof of the nasopharynx, is noncapsulated, and is covered with respiratory epithelium. The adenoids increase in size after birth and usually atrophy by puberty. The palatine tonsils are oval lymphoid masses that lie in the tonsillar fossae, capsulated by the pharyngobasilar fascia, and lined by stratified squamous epithelium. The lingual tonsil tissue located in the base of the tongue is last to develop and persists into adult life. Conventionally, adenoidal size has been assessed using high kilovoltage lateral soft tissue films of the neck (Fig. 45.1), but flexible fiberoptic examination of the nasopharynx has become the gold standard (Fig. 45.2). Assessing the degree of adenoidal hypertrophy involves consideration of the size of the adenoid relative to the choanal openings. An obstruction of the nasopharynx > 50% or an adenoid-to-choana ratio > 0.6 is usually associated with symptomatic obstruction.1–3 Flexible fiberoptic endoscopy helps to rule out other causes of nasal/nasopharyngeal obstruction, such as choanal narrowing, polypoid disease, posterior turbinate hypertrophy, and nasopharyngeal neoplasms that may be missed on traditional radiographs. Fig. 45.1 X-ray showing adenoidal hypertrophy. Fig. 45.2 Endoscopic picture showing adenoidal hypertrophy. Adenoid regrowth should be suspected in patients with recurrent symptoms of nasal obstruction, that is, snoring, mouth breathing, and/or hyponasal speech. The incidence of symptomatic adenoidal regrowth is unknown, but it is felt to be very low. In the study by Buchinsky et al, only 1 in 175 (0.6%) patients developed adenoidal regrowth after adenoidectomy that required revision surgery.4 In the same study, 46 had at least one symptom suggestive of nasopharyngeal obstruction, out of which 35 underwent a flexible fiberoptic nasopharyngeal examination that revealed < 40% nasopharyngeal obstruction in all patients.
Anatomy of the Nasopharynx, Oropharynx, and Waldeyer Ring
Examination of the Nasopharynx
Adenoid Regrowth
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


