Retinopathy of Prematurity and Pediatric 25-Gauge Vitrectomy
 Retinopathy of prematurity (ROP) is a disease of premature, low-birth-weight infants that is characterized by the presence of peripheral avascular retina, neovascularization at the junction of the vascular to the avascular retina, and cicatricial traction on the retina with subsequent traction retinal detachments. ROP has a distinct epidemiology worldwide that depends on the availability of sophisticated neonatal intensive care units (NICUs), trained ophthalmologists for screening and treatment, adequate coordination of services, and obstetrical care. In general, ROP is not a significant problem in countries where the lack of intensive neonatal services leads to poor survival of very low-birth-weight infants, as in certain countries in sub-Saharan Africa. Moving up in the economic development, middeveloped countries, such as many countries in Latin America and Eastern Europe, have a high incidence of severe ROP, given that NICUs are available, but tight postnatal oxygen control, sufficiently trained ophthalmic consultants, and adequate coordination of services are difficult to provide. Whereas ROP had decreased in incidence in the United States as neonatal services had improved and coordination with ophthalmologists trained in screening and treatment of ROP had been achieved, two issues are increasing the incidence of the disease: (a) increased survival of extremely low-birth-weight infants, who commonly develop ROP, and (b) increased incidence of multiple pregnancies (twins, triplet, quadruplet pregnancies), in large part due to aggressive fertility treatments and in vitro fertilization (1). A more recent problem is that ophthalmologists willing and able to treat ROP are becoming less common due to fears of liability and due to the practical concerns of coordinating an ROP service.
Retinopathy of prematurity (ROP) is a disease of premature, low-birth-weight infants that is characterized by the presence of peripheral avascular retina, neovascularization at the junction of the vascular to the avascular retina, and cicatricial traction on the retina with subsequent traction retinal detachments. ROP has a distinct epidemiology worldwide that depends on the availability of sophisticated neonatal intensive care units (NICUs), trained ophthalmologists for screening and treatment, adequate coordination of services, and obstetrical care. In general, ROP is not a significant problem in countries where the lack of intensive neonatal services leads to poor survival of very low-birth-weight infants, as in certain countries in sub-Saharan Africa. Moving up in the economic development, middeveloped countries, such as many countries in Latin America and Eastern Europe, have a high incidence of severe ROP, given that NICUs are available, but tight postnatal oxygen control, sufficiently trained ophthalmic consultants, and adequate coordination of services are difficult to provide. Whereas ROP had decreased in incidence in the United States as neonatal services had improved and coordination with ophthalmologists trained in screening and treatment of ROP had been achieved, two issues are increasing the incidence of the disease: (a) increased survival of extremely low-birth-weight infants, who commonly develop ROP, and (b) increased incidence of multiple pregnancies (twins, triplet, quadruplet pregnancies), in large part due to aggressive fertility treatments and in vitro fertilization (1). A more recent problem is that ophthalmologists willing and able to treat ROP are becoming less common due to fears of liability and due to the practical concerns of coordinating an ROP service.The basic premise that this chapter will try to convey is that, beyond the specific technical details of vitreous microsurgery, the most cost effective and reliable way to decrease ROP blindness is determined by (a) adequate coordination of screening services and (b) timely and appropriate laser treatment for active ROP disease. Vitrectomy surgery should be viewed as salvage therapy for selected cases.
NORMAL RETINAL DEVELOPMENT
Retinal Vascular Development
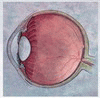
To understand the pathophysiology of ROP, we must start with a basic framework of normal retinal vascular development. Mesenchymal spindle cells grow from the optic nerve toward the retinal periphery and differentiate centrifugally into retinal blood vessels. Vasculature development starts at the optic nerve at gestational age 16 weeks. Retinal blood vessels reach the nasal ora serrata at week 36. Infants born before full retinal vascular development have peripheral retinas devoid of fully developed blood vessels.
PATHOPHYSIOLOGY OF RETINOPATHY OF PREMATURITY
Vascular Endothelial Growth Factor in Normal Retinal Vascular Development
Vascular endothelial growth factor (VEGF) is one of the major molecules involved in retinal vascular development and is critical in the pathophysiology of ROP. Normal VEGF production is required for vascular development. Both phases of ROP have dysregulation of VEGF.
Directional Vasculogenesis
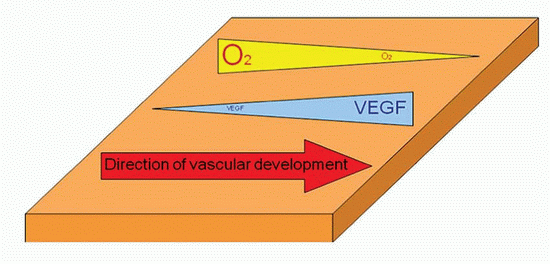
An important aspect of retinal vascular development is its “directionality.” In other words, vessel development has to progress from the nerve toward the periphery. Although the
biological details of vessel development are beyond the scope of this book, some simple concepts should be understood. The VEGF gene promoter has “hypoxia response elements” that bind hypoxia-induced factors (2). This creates a feedback loop that increases VEGF production in hypoxic tissues and decreases VEGF levels as tissue oxygen levels increase. This relation between hypoxia and VEGF also plays a role in diabetic retinopathy, sickle cell retinopathy, and other ischemic retinopathies. In the developing retina, areas absent of blood vessels are relatively hypoxic in comparison to vascularized retina. This creates a gradient of VEGF concentrations that provide the “directional signal,” akin to chemotaxis, for blood vessel development.
biological details of vessel development are beyond the scope of this book, some simple concepts should be understood. The VEGF gene promoter has “hypoxia response elements” that bind hypoxia-induced factors (2). This creates a feedback loop that increases VEGF production in hypoxic tissues and decreases VEGF levels as tissue oxygen levels increase. This relation between hypoxia and VEGF also plays a role in diabetic retinopathy, sickle cell retinopathy, and other ischemic retinopathies. In the developing retina, areas absent of blood vessels are relatively hypoxic in comparison to vascularized retina. This creates a gradient of VEGF concentrations that provide the “directional signal,” akin to chemotaxis, for blood vessel development.
|
Phase 1 of ROP: Arrest of Normal Vascular Development
The association of ROP and O2 became clear after 10,000 babies had vision loss in the 1940s due to aggressive O2 therapy. In 1956, clinical trials demonstrated 3× risk of ROP in babies with O2 supplementation (3). The incidence of ROP decreased after O2 therapy was strongly discouraged in the late 1950s, but NICU mortality increased concurrently.
The intrauterine environment has a PaO2 of 22 to 24 mm Hg, whereas the human adult has an arterial PaO2 of 70 to 90 mm Hg. In essence, the intrauterine environment is relatively hypoxic. In addition, many very low-birth-weight premature babies have pulmonary disease that requires hyperoxic therapy for survival. This hyperoxic environment provides retinal oxygenation of the thin premature avascular retina through the subjacent choriocapillaris and abolishes the hypoxic-driven VEGF gradient required for normal retinal vascular development.
Phase 2 of ROP: Retinal Neovascularization
Weeks after birth, when growth of the eye and retina increase oxygen demand and the choriocapillaris cannot supply enough oxygen to keep up with this increased demand, the peripheral avascular and ischemic retina becomes hypoxic. While the initial phase of ROP depended on decreased VEGF production, the second phase of ROP is caused by pathologically high levels of VEGF secondary to peripheral retinal hypoxia. As in other forms of proliferative retinopathies, such as diabetes, the increased concentration of vitreous VEGF leads to retinal neovascularization. In ROP, the localization of the neovascularization is at the border of the vascular and avascular retina.
Development of Traction Retinal Detachment
Cicatricial regression of the retinal neovascularization leads to retinal traction and secondary traction retinal detachment. An understanding of the vectors of traction is important to surgical relief of traction and repair of the retinal detachments. The origin of all traction vectors is the circumferential ring of retinal neovascularization at the ridge between the vascular and the avascular retina. From this point, the traction, as in the anterior loop traction (radial vitreous collagen fibers) in proliferative vitreoretinopathy (PVR), is directed toward the anterior vitreous base, the lens, and the diametrically opposite neovascular ridge. Since these infants do not have a posterior vitreous detachment, another vector that can play a role in traction is directed from the ridge to the posterior pole and optic nerve.
MANAGEMENT OF THE ROP INFANT
The CryoROP study demonstrated that ROP was amenable to successful therapy through ablation of the peripheral avascular retina (4). It defined threshold disease as retinal neovascularization (stage 3 ROP), in 5 contiguous or 8 total clock hours and plus disease, and it determined that cryotherapy for this level of disease decreased blindness approximately 25%. Since the CryoROP study, despite the absence of large multicenter, randomized trials, laser therapy has largely replaced cryotherapy. A significant caveat of the CryoROP trial was that it was not directed toward determining different clinical levels of disease progression and lumped zone 1 disease infants with zone 2 disease infants. It is now clear that zone 1 disease, since by definition has a larger proportion of avascular to vascularized retina and occurs in the most immature of babies, has a worse prognosis than zone 2 disease and therefore requires earlier intervention. The Early Treatment of Retinopathy of Prematurity Study (ETROP) trial demonstrated that simpler and earlier guidelines for therapy, based mostly on the presence of plus disease (retinal blood vessel dilation and tortuosity at the posterior pole) and/or neovascularization at zone 1, led to improved outcomes (5). Plus disease in particular has become the main focus of clinical determination of vascularly active ROP disease. Despite a degree in subjectivity is accepted in the diagnosis of plus disease, the biological implication is clear. Since the junctional neovascular ridge acts as an arteriovenous shunt, increased shunting through the ridge increases retinal venous blood flow and congestion. Venous congestion at the posterior pole can then be used as a clinical surrogate for determining the magnitude of shunting through the ridge and likelihood of progression of the disease.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


