Purpose
To examine the retinal displacement following successful macular hole (MH) surgery with internal limiting membrane (ILM) peeling and gas tamponade, and to determine the correlation between the extent of displacement and the basal MH size.
Design
Retrospective, interventional, observational case series.
Methods
The medical records of consecutive patients with an idiopathic MH that had undergone vitrectomy with ILM peeling and gas tamponade were studied. The distances between the optic disc and the intersection of 2 retinal vessels located nasal or temporal to the fovea were measured manually preoperatively (A), and 2 weeks and 1, 3, 6, and 12 months postoperatively (B), on the fundus autofluorescence or near-infrared images. The basal and minimum diameters of the MHs were measured in the spectral-domain optical coherence tomographic images. The correlations between the ratio of the retinal displacement (A − B/A) and basal diameters of the MHs were determined.
Results
Twenty-one eyes of 21 patients (9 men, mean age: 64.6 ± 8.4 years) were studied. Ten eyes (47.6%) had stage 2 MH, 9 eyes (42.9%) had stage 3 MH, and 2 eyes (9.5%) had stage 4 MH. The temporal retinal vessels were displaced 260.8 ± 145.8 μm toward the optic disc at 2 weeks postoperatively, which was significantly greater than the 91.1 ± 89.7 μm of the nasal retinal vessels (paired t test, P < .001). The ratio of retinal displacement in the temporal field at 2 weeks was significantly correlated with the basal diameter of the MH (Spearman’s rank correlation coeffieient = −0.476, P = .033.
Conclusions
The greater displacement of the temporal retina than the nasal retina toward the optic disc postoperatively suggests that the temporal retina is more flexible and can be retracted toward the optic disc during the MH closure.
It is well established that pars plana vitrectomy, internal limiting membrane (ILM) peeling, and gas tamponade will lead to high rates of idiopathic macular hole (MH) closure. It has been suggested that the release of vitreoretinal traction by ILM peeling allows the flexible retina to retract toward the optic disc. The recent findings that pharmacologic vitreolysis can lead to a closure of an MH without surgery supports the idea that the primary cause of MH is vitreomacular traction. Analyses of spontaneously or surgically closed MHs suggested that the superficial layers of the sensory retina were the first to reattach during the process of MH closure. If the retina retracts to compensate for an MH at the fovea, then it is likely that the retina will be displaced after successful MH surgery. The degree of displacement should then depend on the size of the MH and should be larger if the MH is large.
Thus, the purpose of this study was to determine whether the retina is differentially displaced after vitrectomy with internal limiting membrane peeling in eyes with an MH. To accomplish this, we measured the distance between the optic disc and an intersection of blood vessels in the temporal and in the nasal retina preoperatively and postoperatively. We also determined whether the degree of displacement was significantly correlated with the size of the preoperative MH.
Methods
This was a retrospective, interventional, observational case series study. We studied the medical records of 21 consecutive patients who had undergone successful vitrectomy for an idiopathic MH at the Teikyo University School of Medicine, University Hospital Mizonokuchi, from August 4, 2011 to March 14, 2013. The procedures used to treat the patients and the examination of their medical records was approved by the Institutional Review Board of the Teikyo University School of Medicine.
Cases with any ocular complications that could affect visual function, such as diabetic retinopathy, macular degeneration, myopic chorioretinal atrophy, rhegmatogenous retinal detachment, cataract >grade III in the Emery-Little scale, and corneal diseases, were excluded. An idiopathic MH was diagnosed and classified as reported by Gass.
Standard 3-port vitrectomy with 23 gauge instruments was performed on 20 eyes and with 25 gauge instruments on 1 eye by a single surgeon to repair the MH. After completion of core vitrectomy, a posterior vitreous detachment was created with active aspiration if one was not present. The ILM was peeled by grasping the ILM with vitreoretinal forceps without the use of dyes to make the ILM more visible, except in 1 eye, in which 0.125% indocyanine green was used. The ILM was grasped at the upper right to the fovea within the vascular arcade and peeled to the edge of the vascular arcade (approximately 2 or 3 disc diameters). After air–fluid exchange, 20% sulfur hexafluoride was used for tamponade. Patients were instructed to maintain a face-down position for 1 day and then allowed to assume any body position except a face-up position until the gas disappeared.
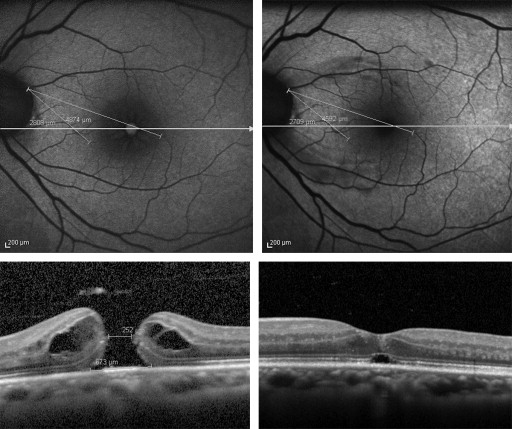
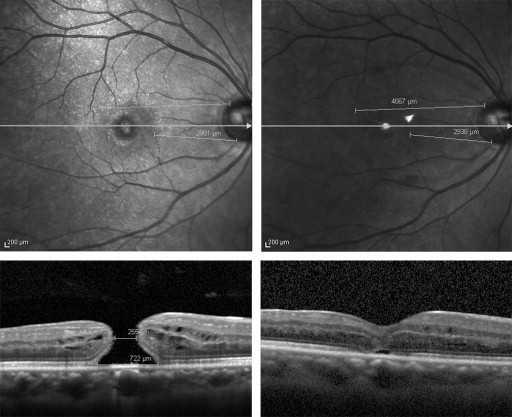
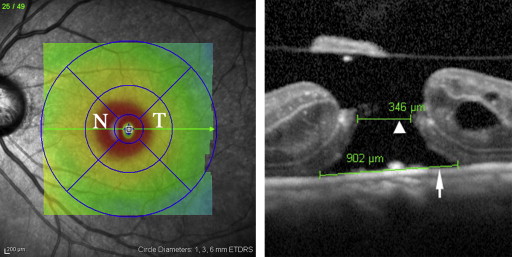
Spectral-domain optical coherence tomography (SD OCT, Spectralis; Heidelberg Engineering, Heidelberg, Germany) was used to evaluate the size and shape of the MH preoperatively and postoperatively. The distance between the temporal margin of the optic disc and an intersection of retinal vessels was measured using the caliper function of the SD OCT preoperatively (A) and 2 weeks and 1, 3, 6, and 12 months postoperatively (B). Fundus autofluorescence (FAF, Figure 1 ) and near-infrared ( Figure 2 ) images were used to measure the distance between the optic disc and the intersection of the retinal vessels. We selected 2 intersections of retinal blood vessels in each eye. One was in the temporal ETDRS subfield and the other was in the nasal ETDRS subfield ( Figure 3 left). The basal diameter and minimum diameter of the MH were measured in the SD OCT images ( Figure 3 right).
Statistical analyses were performed using Excel (Microsoft, Washington, DC, USA) with add-in statistical software (SSRI, Tokyo, Japan). The descriptive data are presented as the means ± standard deviations. The best-corrected visual acuity (BCVA) was measured with a Landolt C chart in decimal units and then converted to logarithm of the minimal angle of resolution (logMAR) units. Paired t tests were used to determine whether differences over time were significant. The correlations between the MH size and distances of the retinal displacement were determined by Spearman rank correlations. A P value < .05 was considered significant.
Results
The medical records of 21 eyes of 21 patients (9 men, mean age, 64.6 ± 8.4 years) with MH were studied. Ten eyes (47.6%) had stage 2 MH, 9 eyes (42.9%) had stage 3 MH, and 2 eyes (9.5%) had stage 4 MH. The average basal diameter of the MHs was 662.1 ± 238.1 μm with a range of 281–1116 μm. The minimum diameter of the MH was 271.8 ± 111.3 μm with a range of 63–459 μm. The mean postoperative follow-up period was 11.0 ± 5.6 months with a range of 3-19 months. The preoperative refractive error (spherical equivalent) was −1.5 ± 3.0 diopters (D). The clinical demographics of all of the participants are summarized in the Table .
| Case No | Age | Sex | Stage | DT (μm) | DN (μm) | Migration Length at 2 Weeks After Surgery (μm) | Best-Corrected Visual Acuity (logMAR) | Basal Diameter (μm) | Minimum Diameter (μm) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 2 Weeks | Baseline | 2 Weeks | Temporal | Nasal | Preoperative | Best Postoperative | ||||||
| 1 | 76 | M | 2 | 4739 | 4353 | 2982 | 2822 | −386 | −160 | 0.699 | 0.155 | 606 | 251 |
| 2 | 71 | F | 2 | 5140 | 4916 | 3219 | 3146 | −224 | −73 | 0.699 | 0.155 | 811 | 275 |
| 3 | 63 | M | 2 | 4999 | 4680 | 2151 | 2027 | −319 | −124 | 1.046 | 0.097 | 983 | 459 |
| 4 | 62 | F | 2 | 5217 | 5110 | 3189 | 3159 | −107 | −30 | 0.523 | 0 | 374 | 181 |
| 5 | 65 | M | 3 | 4875 | 4665 | 2589 | 2590 | −210 | 1 | 1 | 0 | 690 | 232 |
| 6 | 49 | F | 3 | 5035 | 4667 | 2981 | 2936 | −368 | −45 | 0.699 | 0.145 | 722 | 255 |
| 7 | 56 | F | 4 | 4369 | 3886 | 1795 | 1752 | −483 | −43 | 0.523 | 0.097 | 894 | 387 |
| 8 | 65 | M | 2 | 4679 | 4414 | 2367 | 2314 | −265 | −53 | 1 | 0.301 | 951 | 114 |
| 9 | 62 | F | 2 | 5289 | 5109 | 3201 | 3141 | −180 | −60 | 0.699 | 0.145 | 587 | 378 |
| 10 | 75 | M | 3 | 4353 | 4062 | 2462 | 2406 | −291 | −56 | 1.097 | 0.155 | 902 | 346 |
| 11 | 71 | F | 3 | 5000 | 4714 | 2305 | 2256 | −286 | −49 | 1 | 0.523 | 1116 | 443 |
| 12 | 65 | F | 2 | 4717 | 4501 | 2977 | 2882 | −216 | −95 | 0.398 | 0.155 | 344 | 168 |
| 13 | 62 | F | 3 | 4863 | 4632 | 2920 | 2862 | −231 | −58 | 1.097 | 0.097 | 701 | 368 |
| 14 | 73 | M | 3 | 4347 | 4277 | 2738 | 2754 | −70 | 16 | 0.398 | 0.398 | 281 | 112 |
| 15 | 76 | F | 2 | 4937 | 4619 | 2790 | 2474 | −318 | −316 | 0.398 | 0.046 | 403 | 63 |
| 16 | 65 | M | 3 | 4045 | 3951 | 2732 | 2706 | −94 | −26 | 0.699 | 0.301 | 725 | 315 |
| 17 | 75 | M | 2 | 4786 | 4855 | 2193 | 2187 | 69 | −6 | 0.699 | 0.046 | 447 | 244 |
| 18 | 46 | F | 3 | 4674 | 4066 | 2458 | 2155 | −608 | −303 | 0.523 | −0.079 | 703 | 306 |
| 19 | 59 | M | 2 | 5403 | 5047 | 2987 | 2793 | −356 | −194 | 0.824 | 0.398 | 707 | 390 |
| 20 | 57 | F | 4 | 5911 | 5659 | 3005 | 2865 | −252 | −140 | 0.398 | 0.155 | 285 | 169 |
| 21 | 63 | F | 3 | 4874 | 4592 | 2808 | 2709 | −282 | −99 | 1 | 0.301 | 673 | 252 |
| Mean | 64.6 | 4869.1 | 4608.3 | 2707.1 | 2616 | −260.8 | −91.1 | 0.733 | 0.171 | 662.1 | 271.8 | ||
| ± SD | 8.4 | 412.1 | 432.9 | 388 | 389.4 | 145.8 | 89.7 | 0.251 | 0.15 | 238.1 | 111.3 | ||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


