and Mitrofanis Pavlidis2
(1)
Department of Ophthalmology, Uppsala University Hospital, Uppsala, Sweden
(2)
Augencentrum Köln, Cologne, Germany
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-319-20236-5_20) contains supplementary material, which is available to authorized users.
Electronic supplementary material
for this chapter is accessible online at http://extras.springer.com/ by searching via the ISBN.
20.1 General Introduction
Video 20.1: PVR detachment
Video 20.2: Peeling techniques for PVR detachment
Video 20.3: PVR peeling
Video 20.4: PVR detachment secondary to trauma
Video 20.5: Traumatic detachment
The correct assessment and practical management of PVR retinal detachment is one of the biggest challenges in vitreoretinal surgery. The usage of an encircling band for PVR detachment was standard only 10 years ago. Today, the usage of an encircling band has drastically reduced (in our department) to approximately 2–5 cases per year. There are many causes for this development: the surgery today is less traumatic, the primary detachment surgery is more successful resulting in less severe PVR cases and, not last but least, the advent of new agents such as heavy silicone oil. Heavy silicone oil is an excellent instrument for the difficult inferior detachments.
PVR consists of epiretinal PVR, subretinal PVR and intraretinal PVR. Subretinal PVR and epiretinal PVR can be removed with peeling. Intraretinal PVR results in shortening of the retina and can only be treated with retinectomy or encircling band or the usage of silicone oil (see Flow chart 20.1).
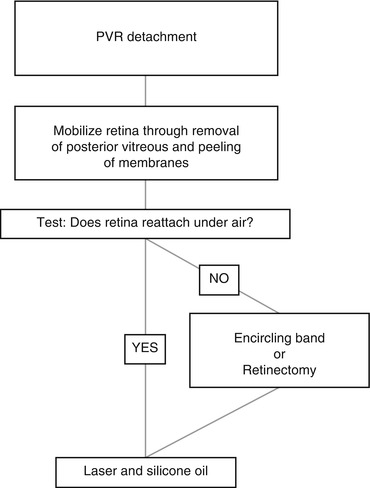
Flow chart 20.1
Our treatment algorithm for PVR detachments. If you use an encircling band, you can use often a gas tamponade. If you perform a retinectomy, you need in most cases silicone oil. If you do not perform encircling band and not retinectomy, then you need in the most cases light silicone oil for the superior detachment and 2–4 weeks later heavy silicone oil for the inferior detachment
There are two typical cases for PVR detachment:
1.
Old and total PVR detachment
2.
PVR redetachment
Our surgical approach for an old detachment is removal of vitreous with posterior vitreous + membrane peeling + cerclage or retinectomy + laser + silicone oil (in most cases light 1000 cSt silicone oil). If you do not use cerclage or retinectomy, then quite a few cases develop an inferior detachment. In this case, we extract the light silicone oil and inject heavy silicone oil.
Our surgical approach for a PVR redetachment is removal of condensated posterior vitreous (if present) + membrane peeling + laser + silicone oil (in most cases light 1000 cSt silicone oil). In case of an inferior redetachment, we extract the light silicone oil and inject heavy silicone oil.
The first surgical step in PVR retinal detachment is the removal of membranes. This means peeling, peeling and peeling. In order to perform a good peeling, we like to stain the membranes. Because many membranes are located in the periphery, the usual method does not work well. We therefore make a fluid–air exchange and then drop the dye on the PVR membranes in an air-filled eye. The dye is very concentrated on these areas, and you always get a good staining of the membranes. Return to a fluid-filled eye and start with the peeling on the posterior pole and work from there to the ora serrata.
The next main step is the treatment of intraretinal PVR. There are three tools against intraretinal PVR with shortening of the retina:
1.
Cerclage
2.
Retinectomy
3.
Light and heavy silicone oil
This surgery can be performed with hybrid technique (one 27G infusion trocar and two 25G instrument trocars) or only with 27G.
Instruments
1.
Hybrid 3-port trocar with chandelier light
2.
120D lens, for peeling: 90D lens
3.
Vitreous cutter
4.
Endodiathermy
5.
Endolaser
6.
Backflush instrument
7.
Scleral depressor
8.
Membrane pic
9.
Eckardt endgripping forceps or serrated jaw forceps
10.
Intravitreal scissors (curved or straight)
If available
11.
25G knob spatula
12.
23G serrated jaw forceps
13.
27G Atkinson cannula
Dye
Trypan blue
Tamponade
Intraoperative: PFCL
Postoperative: light and heavy silicone oils and occasionally long-acting gases
Individual Steps
1.
Hybrid 3-port system with chandelier light
2.
Phacoemulsification
3.
Vitrectomy
4.
Staining of the membranes with trypan blue
5.
Peeling of PVR membranes
6.
Assess if the retina attaches under air or PFCL
7a.
Encircling band
7b.
Retinectomy
8.
Photocoagulation of breaks
9.
Prepare anterior chamber for tamponade
10a.
PFCL × silicone oil exchange
10b.
PFCL × air exchange
11.
Tamponade
12.
Removal of the trocars
20.1.1 The Surgery Step by Step: Figs. 20.1, 20.2, 20.3, 20.4, 20.5, 20.6, 20.7, 20.8, 20.9, 20.10, 20.11, 20.12, 20.13, 20.14, 20.15, 20.16, 20.17, 20.18, 20.19, 20.20, 20.21, 20.22, 20.23, 20.24, 20.25 and 20.26

Fig. 20.1
A posteriorly closed funnel. Remove the attached posterior vitreous in order to relax the retina
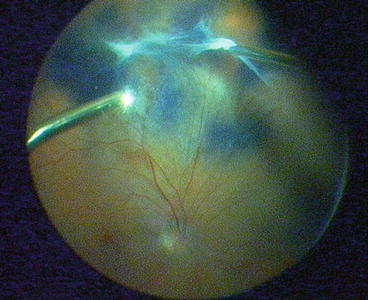
Fig. 20.2
Remove the posterior hyaloid up to the ora serrata in order to mobilize the retina
Fig. 20.3
An air-filled eye. Stain membranes in the centre and periphery with trypan blue
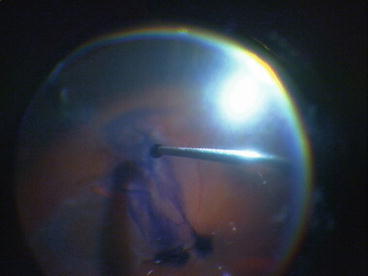
Fig. 20.4
Drop the dye onto the membranes to achieve maximal concentration
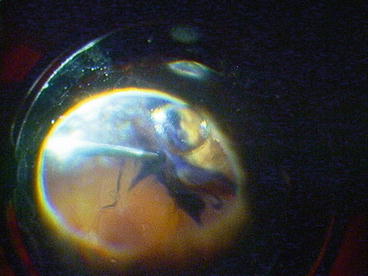
Fig. 20.5
Even peripheral membranes can be stained with this technique. This is not possible in a BSS-filled eye
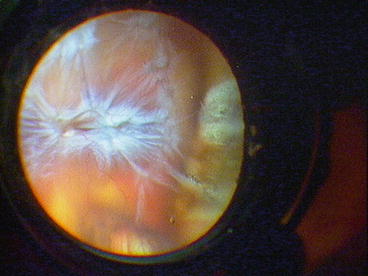
Fig. 20.6
An eye with a tractive PVR detachment
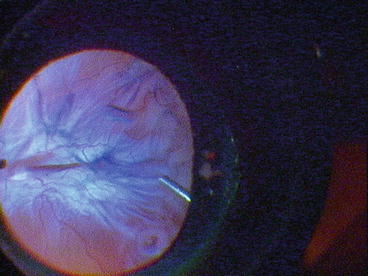
Fig. 20.7




The membranes are well stained with trypan blue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
