CHAPTER 60 Retinal detachment and PVR

Epidemiologic considerations and terminology
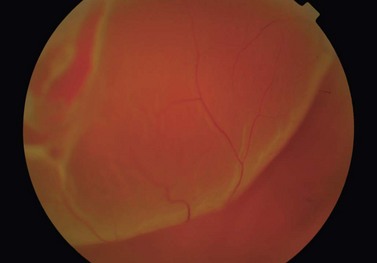
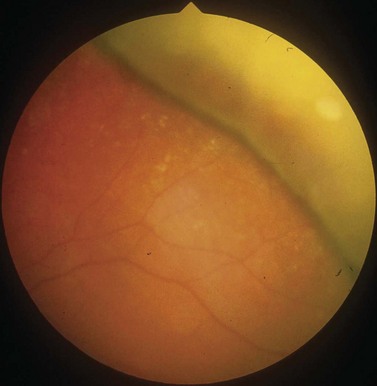
In the majority of cases, the retinal detachment is due to fluid which gains access to the subretinal space via a retinal hole, so called rhegmatogenous retinal detachment (RRD) (Fig. 60.1). In non-rhegmatogenous detachment the separation arises from serous exudation, or for other reasons, and will not be considered further in this chapter.
RRD affects about one in 10 000 adults annually1, and has a higher incidence in myopes2, pseudophakes3, and following trauma4.
Anatomical considerations
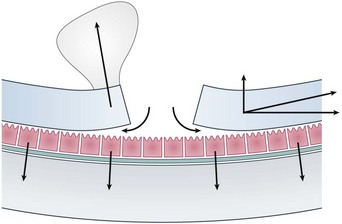
The subretinal space is a potential one, normally kept dry by the pumping action of RPE cells. If the rate of fluid flow through a retinal hole is greater than the rate at which it can be pumped out, then RRD occurs. The balance between ingress and outflow of fluid can be affected by a number of different factors (Fig. 60.2). Dynamic traction from the vitreous, for example following a PVD, can rapidly accelerate the progression of retinal detachment. Similarly increased concavity in the case of a posterior staphyloma, combined with a presumed reduction in the quality of the RPE pump in high myopes, can produce retinal detachments from macular holes, which do not otherwise occur in macular hole patients.
Retinal holes can be classified into three groups: (i) round holes; (ii) traction, or ‘U’ tears; and (iii) other breaks. Round holes are very common, but rarely lead to RRD5. They are usually associated with patches of lattice degeneration. In a small subset of young myopic patients, they can cause slowly progressive retinal detachment, accounting for approximately 5% of patients requiring treatment. The majority of RRDs are caused as a result of one or more traction, or ‘U’ tears secondary to a PVD. The most common location for such tears is the superior temporal quadrant.
Fundamental principles
The principle of treatment for RRD is prevention of fluid flow through the retinal hole. This can be achieved by closing then sealing the hole. Closure of the hole refers to the apposition of retina and underlying RPE, closing the gap between them. Sealing of the retinal hole refers to the creation of a permanent adhesion between the retina and the underlying tissue. As current methods of sealing require the passage of time, it is usual to combine sealing with temporary closure, thus keeping the edges of the hole apposed until the adhesion has developed. Buckles work by creating an indentation of the sclera, thereby closing holes, but also creating a convex surface in favor of re-attachment6. Tamponade with gas or silicone oil blocks the retinal hole by surface tension, preventing fluid flow through it. Both cryotherapy and laser create tissue injury which results in chorioretinal adhesion 5–10 days later.
Preoperative assessment
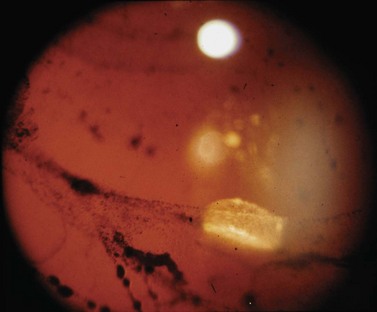
The aim of preoperative assessment is to confirm the diagnosis, identify the retinal holes, and plan the most appropriate surgical technique. Although the vast majority of patients presenting with retinal detachments have RRD, the possibility of an exudative retinal detachment must always be considered, particularly if a retinal hole is not seen. The presence of pigment cells in the anterior vitreous (’tobacco dust’) is strongly correlated with the presence of a retinal hole, though a similar sign can occur as a result of iris trauma during cataract surgery (Fig. 60.3). Examination of the anterior segment is important, as it may give clues to the etiology, but is also helpful in determining the quality of the view that the surgeon will get during surgery.
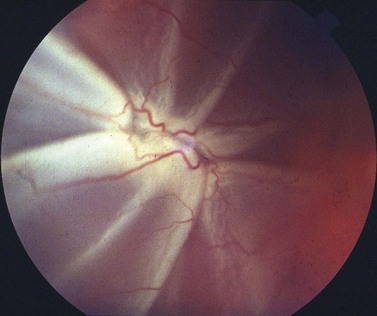
An assessment of the degree of proliferative vitreoretinopathy (PVR) should also be made. The proximity of ‘star folds’ near retinal breaks may mean that vitrectomy is required (Fig. 60.4). Contraction of the vitreous base may be an indication for an encircling buckle.
Operation techniques
Scleral buckling
Scleral buckling is a surgical procedure in which indentation of the scleral surface is achieved by suturing a silicone support to the sclera, thus sealing the retinal break, relieving vitreoretinal traction and reducing the flow of fluid into the subretinal space (Fig. 60.5). When combined with retinopexy, chorioretinal adhesion results maintaining retinal reattachment even when the indent subsequently fades.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


