12 Results of Endoscopic Sinus Surgery: Personal Experience
Introduction
Looking back on 30 years of intense active involvement in endoscopic sinus surgery, I have to admit many advances and refinements but must also affirm that the initial concepts of indication and technique have retained their validity. One has to realize, though, that reading the contemporary literature will disclose such a broad spectrum of different attitudes and techniques that comparison of treatment modalities, even between renowned services, is difficult.
The data given in the literature are difficult to interpret because of the large number of variable factors that infl uence the results, such as referral patterns, indications for surgery, equipment used, and variations in surgical skill. In addition, the results may improve over the course of time, even for the same surgeon. Even more infl uential factors are the criteria of success and failure, and these are seldom the same in different reports. What is “very good,” “good,” and “moderate” in the assessment of treatment of sinusitis? Does these terms refer to the satisfaction of the patient or of the endoscopist? How liberally were the results classified, and for how long were the patients followed-up? Was like compared with like? Were the patients similar with respect to other diseases and risk factors? Were related lesions such as septal deviation, defects of bone or mucosa after previous antral operations, or scarring after previous ethmoid operations taken into account? All these parameters can have a marked effect on the results of a later intervention, so that the choice of a homogeneous group for comparison is not always possible, even in a large series of patients. As a surgeon, I cannot agree with the statisticians’ viewpoint that using a large series of cases from several centers compensates for any bias.
Nonetheless, the publication of results of ESS is essential for decision-making by the informed patient. It will also help the patients to agree on a plan of individualized surgery with a more or less unpleasant period of endoscopic aftercare. And it may, finally, serve as a strong argument for health care organizations not to adopt equipment solely on cost-saving grounds, weighing these costs against greater expenses for a chronically ill person. Furthermore, standard values must be available for family practitioners and other referring colleagues who have to select our specialty among allied disciplines for certain diseases, who must address medico-legal challenges, and who want to provide detailed explanation to their patient.
Nomenclature and classifications are not understood in the same way by different authors. Terms such as partial ethmoidectomy or pansinus operation often cover various extents of surgery, as I have had to learn from many revisions carried out on patients who had been surgically treated elsewhere, since the first edition of this monograph. The extent of flanking septal corrections and conchotomies, for example, is frequently not documented, although these measures can be decisive of success. Also documentation of the exploration and eventual ouverture of the frontal and sphenoidal sinuses is often neglected in surgical steps referred to as pansinus operation. Similar deficiencies of documentation concern postoperative endoscopic aftercare, which, in my experience, contributes to the final outcome almost as strongly as the quality of the intervention itself. Published statistics and related scores are therefore sometimes problematical.
These difficulties in acquisition of hard data can also apply to material from one’s own university teaching department. For this reason, the following retrospective overview is restricted to a consecutive series of practically uniform types of endoscopic surgery for sinus treatment, executed by the same surgeon (Wigand 1990), based on an analysis by two different investigators of interventions performed between 1986 and 1991 (Mrakovcic 2001; Wällisch 2002). This restriction explains the comparatively small number of cases, and is also a clue to the disadvantage of the widespread inhomogeneity in the practice of postoperative care among the referring ENT specialists. With this in mind, the following outline of my own results comprises only three groups of indications:
1. Chronic rhinosinusitis (CRS)
– Partial ethmoidectomies subdivided into (a) first operations and (b) revisions
– Total ethmoidectomies/pansinus operations subdivided into (a) first operations and (b) revisions
2. Endomicroscopic dacryocystorhinostomy according to West
3. Neoplasia
– Inverted papilloma
– Malignancy
All interventions were described in Chapter 6. Their mucosa-preserving character was stressed but, of course, could not be realized uniformly in all cases. In procedures for CRS, flanking septal corrections, especially of regions III and IV, and trimming of the middle turbinate as described in Chapter 6 were always ingredients of partial and total ethmoidectomies if nature had not provided excellent nasal architecture, which is rare. These served (a) to facilitate intraoperative instrumentation, (b) to enhance postoperative healing by increased ventilation, and (c) to facilitate postoperative treatment by making it less painful.
Chronic Rhinosinusitis (CRS)
Intranasal endoscopic sinus surgery for CRS was introduced at the Erlangen University ENT Department in 1975, starting with infraturbinal antrostomy. Endonasal ethmoidectomy followed in 1976. Transethmoidal frontal and sphenoidal sinusotomies were added a year later, and supraturbinal sinusotomy in 1980. The latter became routine from 1983 onwards. Procedures at the anterior skull base such as closure of dural fistula had already been tried in 1976. Other indications such as tumor and orbital complication have followed since 1981.
The following review is based on the author’s own operations (n = 506) from 1986 into 1991, thus representing a quasi-standardized and mature technique, and allowing a follow-up of more than 3 years. It consists of both an evaluation by questionnaire and an endoscopic examination. The figures for both do not tally because many former patients who were approached did not accept the opportunity of the cost-free inspection offered. It became apparent that adequate postsurgical guidance on woundhealing had been implemented in only a minority of cases.
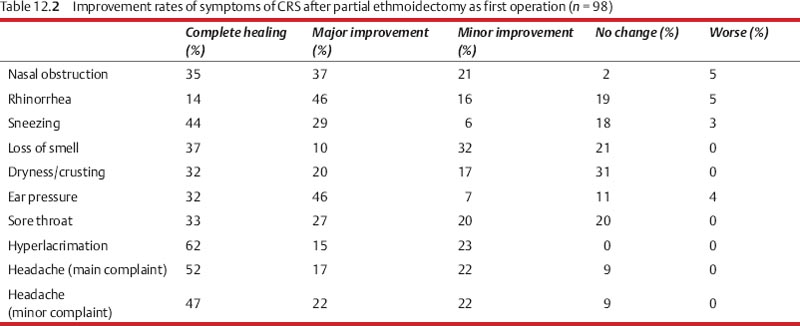
Partial Ethmoidectomy for Initial and Limited Stages of CRS (n = 112)
This procedure included uncinatectomy, opening of the bulla ethmoidalis and of adjacent affected ethmoidal cells, but was terminated in the presence of healthy cells lined with a thin, normal-looking mucosa. It included also a limited supraturbinal nasoantrostomy for inspection of the maxillary cavity.
Nasal obstruction (88%) and rhinorrhea, mostly combined with an unpleasant postnasal drip (72%) were the most frequent complaints of this group. Table 12.1 gives the data on the presenting symptoms.
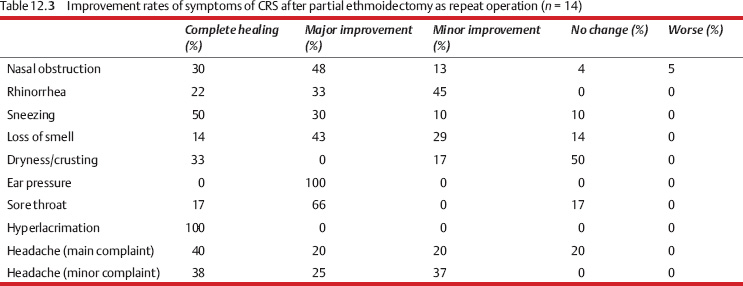
Tables 12.2 and 12.3 give an overview on the postoperative improvement rates of 98 first interventions and 14 revision operations. The mean observation period was 3.7 years (1–6 years). The age of the individuals varied from 12.8 to 72.6 years; 78 were male, 34 were females. One hundred and twelve answered questionnaires were evaluated.
Table 12.4 reports answers of responding patients concerning the long-term necessity of consulting an ENT doctor after surgery.
| Symptoms | Preoperatively (%) |
| Nasal obstruction | 88 |
| Rhinorrhea | 72 |
| Sneezing | 29 |
| Loss of smell | 23 |
| Dryness/crusting | 39 |
| Ear pressure | 27 |
| Sore throat | 41 |
| Hyperlacrimation | 13 |
| Headache (main complaint) | 25 |
| Headache (minor complaint) | 29 |

| Postoperative ratings (%) | |
| Normal mucosa | 70.3 |
| Scarring | 12.5 |
| Cystic formations | 6.3 |
| Thickening of the mucosa | 6.2 |
| Prominent secretions | 3.1 |
| Small polyps | 1.6 |
A more objective evaluation of partial ethmoidectomies as treatment of limited CRS through endoscopic inspection performed by a physician who was not involved in the diagnosis and treatment of this patient concerned the form and placement of the nasal septum and turbinates, the supraturbinal antrostomy, and the aspect of the lining mucosa. Since the inner ethmoidal texture was not directly visible, the findings listed in Table 12.5 apply predominantly to the maxillary antrum. The figures do not highlight that in some cases the postoperative check-up disclosed more severe changes than were observed during surgery!
The nasal septum was in a good medial position (46.6%) or somewhat lateralized (44%), with bridging scar formation in 12.5%. There was no case of intraoperative or postoperative complications (see Chapter 9) in this series. A small symptomless septum perforation had developed in two cases, neither requiring repair.
Total Ethmoidectomy/Pansinus Operation for Disseminated and Diffuse CRS (n = 208)
These subcategories can be grouped together because this procedure was executed for nearly identical indications. The main pathological finding in a preoperative CT series was the complete or near-complete opacifi cation of the ethmoids combined with various degrees of marginal or convex intracavitary shadows (see Chapter 3) in the maxillary, frontal, and/or sphenoidal sinuses. Together with a total ethmoidectomy, the interventions included, at least, a moderate fenestration of these cavities for their endoscopic evaluation and, in some cases, a broader ouverture for intracavitary excisions. Sharp bone resection with preservation of the lining mucosa of opened cells and cavities was a leading characteristic of these procedures, which were mostly combined with sculpting of the middle turbinate and adequate septal correction.
The re-examined material comprised 208 primary cases and 77 revisional cases: 63% male/37% female among first interventions and 71% male/29% female in the group of revisions at an age of 5–79 years with an average of 47 years. Only six patients were younger than 20 years.
While first partial resections of the ethmoid were carried out bilaterally in 96% of the 163 registered patients, bilateral total ethmoidectomies/pansinus operations amounted to 95% (91% in revisions) of the 320 registered candidates. It must be stressed that more than 50% of the secondary attempts concerned individuals who had undergone partial ethmoidectomies before, as functional endoscopic sinus surgery (FESS) in the manner of Messerklinger/Stammberger.
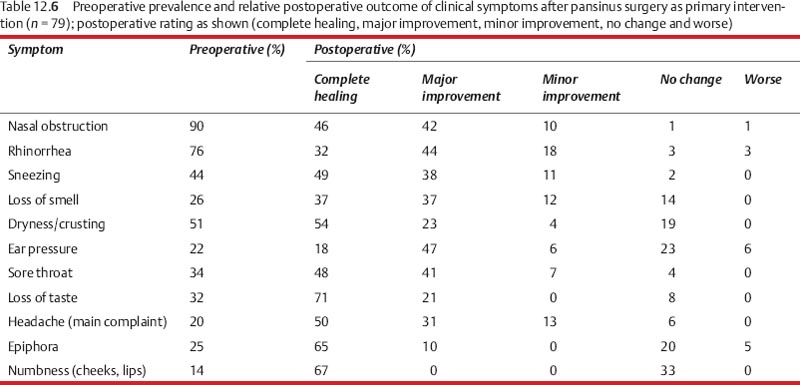
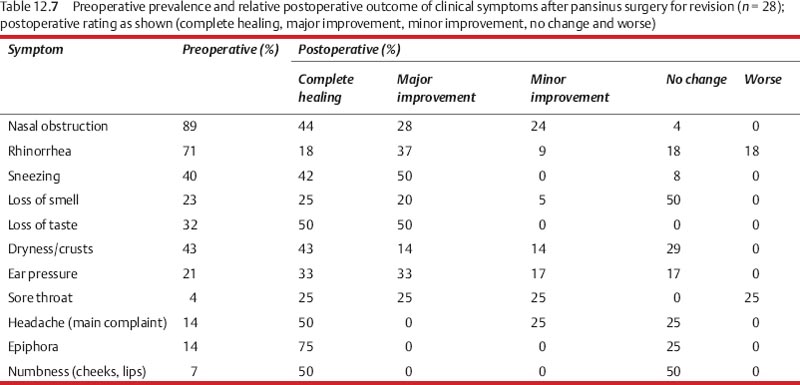
Tables 12.6 and 12.7 indicate the subjective evaluation of both groups after pansinus operation regarding the prevailing symptoms as percentage of the affected individuals. The mean observation period was 3.1 years (1–7 years) and 320 answered questionnaires were evaluated.
The sense of smell before and after ethmoidectomy is a yardstick of the severity of the disease, the effi cacy of treatment, and also the precision of the mucosa-sparing technique. The patients themselves often regard the recovery of a long-absent olfactory function as being more important than the improved nasal respiration and relief from headache. Tables 12.6 and 12.7 present the author’s experience with a consecutive series: The sense of smell was regained in a large proportion of cases, whereas olfactory deterioration was exceptional.
An illuminating example of the pathological mechanism of dysosmia in nasal and ethmoid polyps may be of interest. After a septal correction done elsewhere, a 45-year-old patient complained of loss of the sense of smell due to mechanical occlusion of the olfactory cleft by mucosal swelling and polyps. At the first investigation he was found to have hyposmia (Fig. 12.1a) . When he presented for operation a few months later, he had become anosmic. The entrance to both olfactory clefts was found to be narrowed by scar tissue at follow-up several months after ethmoidectomy (Fig. 12.1b) . At this time the sense of smell was relatively poor, but improved greatly after division of synechiae. A follow-up osmogram (Fig. 12.1c) indicated a return to normal on one side and improvement on the opposite side.
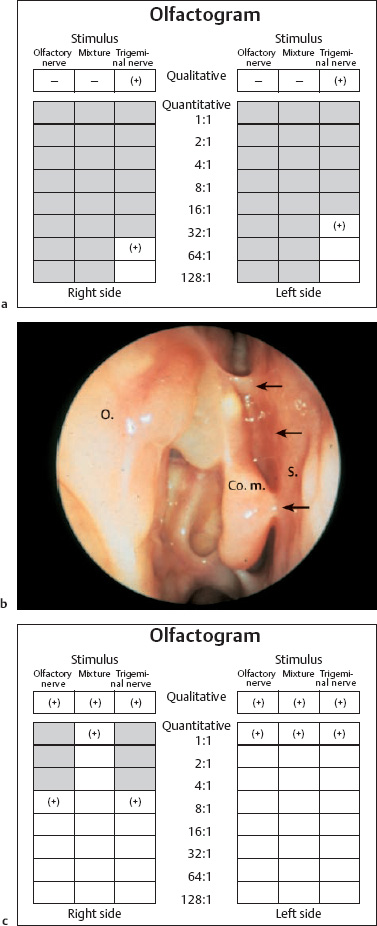
Fig. 12.1 a–c Mechanical obstruction of the right olfactory cleft by bridges of scar tissue.
a Olfactogram of anosmia in chronic polypoid pansinusitis.
b Five months after ethmoidectomy, the olfactory cleft is again partially closed by synechiae (arrow) and the patient again complains of severe hyposmia (70° telescope).
c The sense of smell returned almost completely to normal after endoscopic division of the scar tissue.
Scar formation in the olfactory rim is most detrimental to olfaction. Its most frequent cause is nasal polypectomy with snares tearing valuable mucosa from the middle turbinate and superior septum. Endoscopy often cannot locate the injured area. Undisturbed smell, on the other hand, can remain possible with small remnants of olfactory mucosa (Fig. 12.2)
|
Table 12.8 shows the answers of 170 patients about the long-range necessity of consulting an ENT doctor after pansinus operations. If one takes into account that all of these persons had been permanent outpatients before surgery, one may estimate the increase in quality of life and the cost reduction by an active surgical treatment of CRS, almost approaching the figures for partial ethmoidectomies in Table 12.4.
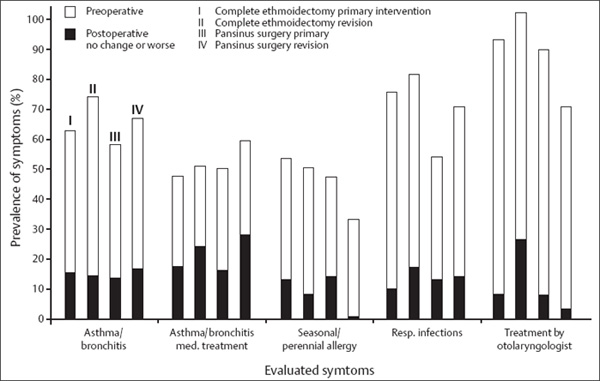
Considering that the nasal and paranasal mucosa is only part of the extensive system of mucociliary epithelium reaching from the nasal entrance into the bronchi and middle ear, some other results concerning allergy and bronchial asthma deserve attention. Figure 12.3 reflects related information from 208 responding patients. It shows high benefits independently of the type of surgical procedure. A clear gain of health was found in more than two-thirds of patients suffering from chronic bronchitis and asthma, whereas approximately 50% of this group still needed some medical help. Similarly, seasonal and perennial allergy as well as respiratory infections decreased by marked percentages.
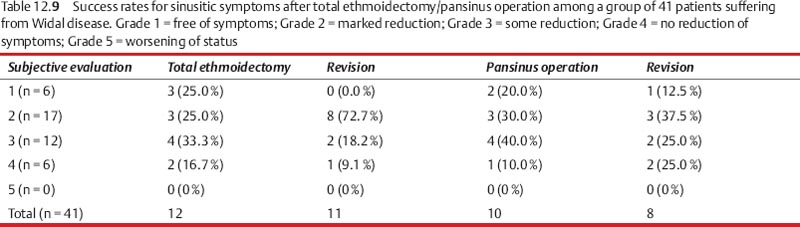
Cases with intolerance to analgesics (Widal disease) were included in the preceding cohorts but, because of their specific mucosal hyperreactivity, were also subjected as a special group of 41 patients to a separate evaluation. Table 12.9 gives the related figures for their postsurgical scales of complaints. Comparing these data with those in Fig. 12.3, which included the Widal patients, a marked reduction of expectations can be read from Table 12.9 for this special condition. Unfortunately, the analysis for the year 2000 did not exclude this unfavorable subgroup, otherwise higher success rates would have been evidenced for the entire population.
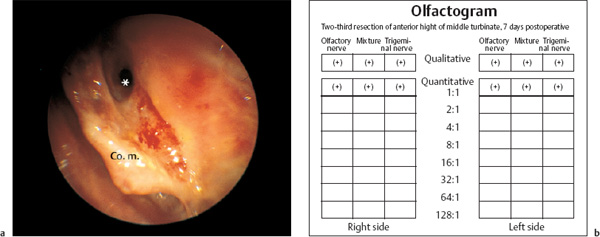
Fig. 12.2 a, b Mechanical stenosis by scar formation in the olfactory rim.
a A flat remnant of the right middle turbinate with a scarred surface on both sides narrows the sensitive area. The enlarged nasofrontal duct stays open (*).
b Normal sense of smell despite the marked reduction of the olfactory epithelium documented in the olfactogram.

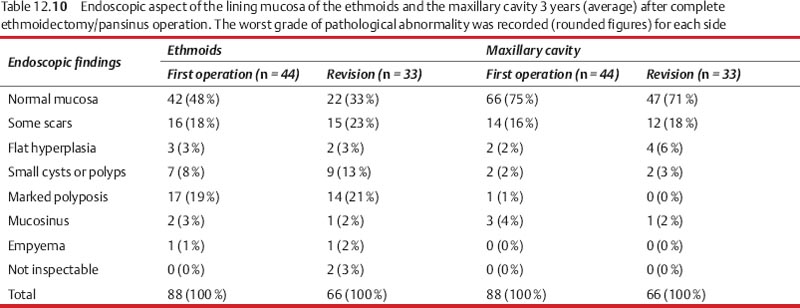
The more objective long-term findings by endoscopic survey of the operated compartments are listed in Table 12.10. This summary of the effects of endoscopic cleansing of the mucosal covering in the paranasal sinuses in advanced chronic-hyperplastic and polypous sinusitis confirms our earlier findings of potential full recovery of severely diseased and structurally altered mucosa (Wigand and Goede 1995), making an absurdity of the earlier notion of its biologically inferior quality (Albrecht; Wittmaack 1918). Taking into account that the loss of vital mucosa from preceding ethmoidectomies with production of extensive scar tissue does not exclude extensive regeneration into a normal-looking mucosal texture (Fig. 12.4a, b) , one must judge the underlying idea of surgery aiming at reventilation and drainage as a fruitful biomechanical interpretation of the pathogenesis. To these observations must also be added that sometimes late pathological efflorescences, absent during surgery, must have developed despite or due to the altered microanatomical conditions.
It must finally be stressed that no case of severe complications was on record; in particular no visual defi cits, injury of the skull base, or tearing of olfactory fibers became evident for the period 1986–1991. Fifty years ago, it was the high proportion of visual defects, blindness, CSF fistulas, and meningitis that brought intranasal ethmoidectomy into disrepute, rather than the poor results. The importance of the introduction of endoscopy thus cannot be overestimated.
The complications in the author’s series for these years were relatively minor, with no permanent injury (Table 12.11). One fatality, however, must be admitted for an earlier period due to an unexpected malformation of the internal carotid artery channel within the sphenoid cavity. This case was described in Chapter 9. Probing of the sphenoid cavitywith a blunt suction tube led to a massive hemorrhage with a critical drop in blood pressure despite packing of the posterior ethmoid area. The patient died 5 days later of bilateral cerebral edema despite immediate anesthesiological support and rapid transfusion. The autopsy showed that the internal carotid artery was protruding deep into the lumen of the sphenoid sinus, and had almost no protective bony covering.
A similarly sized series of operations carried out by more than thirty full-time academic staff and assistants in training in the author’s department included one case of meningitis and brain abscess with fatal outcome, and one case of blindness due to postoperative intraorbital bleeding. The brain abscess presented 2 weeks after the operation, and it was unclear whether it was already present before the operation or was caused by the operation itself. In conclusion, one must admit that even with well-organized training programs a certain learning curve applies and exacts some penalty.
Fig. 12.4 a, b Full recovery of a hyperplastic polypoid mucosa after endoscopic pansinus operation.
a Endoscopic aspect after 2 years.
b A coronal CT image shows the clear ethmoid on the operated left side (*) and opacification in the unoperated right ethmoid.
Table 12.11 Complications after complete ethmoidectomy for diffuse ethmoid polyposis (n = 220)
| Asthma attack immediately after operationa | 4 (1.8%) |
| Neuralgia of face and head | 4 (1.8%) |
| Postoperative anosmia | 2 (0.9%) |
| Intraoperative CSF leak, tearing of olfactory fibers | 2 (0.9%) |
| Orbital hematoma | 1 (0.5%) |
| Ethmoid mucocele | 1 (0.5%) |
| Death | 0 |
| Blindness | 0 |
| Paresis, double vision | 0 |
| Meningitis | 0 |
| Ozena | 0 |
a After pain medication in patients with undiagnosed sensitivity to analgesics.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


