and Charles P. Molumi2
(1)
University of Papua New Guinea and Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
(2)
Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
5.1 Repair of Alar Defect with Full Thickness Skin Graft

Fig. 5.1
Incision site is marked out for nasal basal cell carcinoma excision

Fig. 5.2
The defect after excision

Fig. 5.3
Full thickness skin graft is harvested from the postauricular region

Fig. 5.4
Full thickness post auricular skin graft is used to close the nasal defect

Fig. 5.5
Wound heals without scaring, 10 weeks after operation
5.2 Superior Based Nasolabial Flap for Reconstruction of Alar Defect

Fig. 5.6
The flap is marked out for reconstruct of alar defect using a superior based nasolabial flap
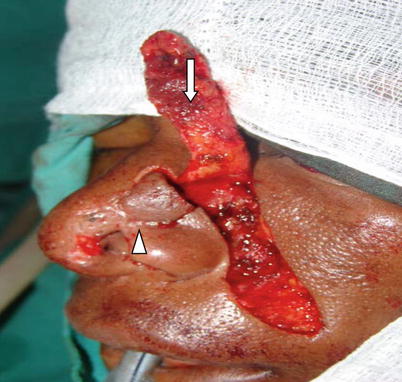
Fig. 5.7
A nasal dorsum turnover flap (arrow head) and a superior based nasolabial flap (arrow) are raised

Fig. 5.8
The nasal dorsum turnover flap is reflected down
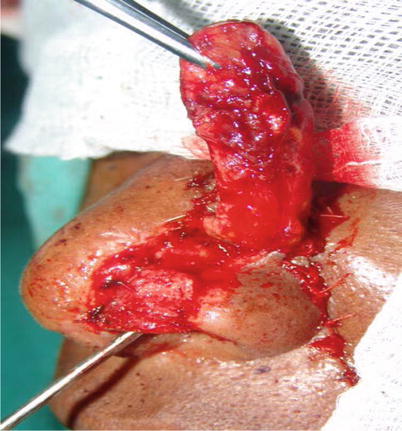
Fig. 5.9
The nasal dorsum turnover flap is stabilized by suturing its lateral and basal sides with the respective parts of the vestibular skin

Fig. 5.10
The donor area of the nasolabial flap is sutured; the nasal dorsum turnover flap forms the roof of the vestibule

Fig. 5.11
The nasolabial flap is sutured with the nasal dorsum and with the turnover flap
5.3 Modified Reiger Glabellar Rotation Flap

Fig. 5.12
The incision is marked out for reconstruction of the alar defect using a Reiger glabellar rotation flap

Fig. 5.13
The entire skin of the nasal dorsum including the glabella and part of the cheek is mobilised. The skin above the defect is used as rotation flap for inner lining

Fig. 5.14
The flap is transported to cover the defect

Fig. 5.15
Appearance of the patient 3 months after operation
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


