Reoperative surgery in the neck for recurrent/persistent well-differentiated thyroid cancer is associated with increased morbidity compared with primary surgery. Reoperative surgery is technically more challenging because of the presence of scar tissue and disruption of the normal fascial planes and anatomy, which may result in a greater risk of injury to nerves and other vital structures. When performing reoperative surgery, an algorithm should be followed that allows for safe and effective removal of recurrent/persistent disease. This algorithm should include a systematic review of prior operative and pathology notes, imaging studies appropriate for localization of disease, an understanding of reoperative central and lateral neck anatomy, along with an appreciation for disease behavior.
The incidence of thyroid cancer in the United States has been increasing over the past several decades. Some attribute this increase to improved detection rates of small papillary cancers with the widespread use of high-resolution ultrasonography in combination with fine-needle aspiration (FNA) biopsy of subcentimeter thyroid nodules. Most well-differentiated thyroid cancers (WDTC) have a favorable prognosis with excellent long-term overall survival. The American Thyroid Association has generated guidelines that help to clarify posttreatment surveillance strategies for patients diagnosed with WDTC. Similar to the observed trend of increased detection rates of smaller papillary cancers, sensitive assays including ultrasonography and monitoring of serum thyroglobulin levels have ushered in a new era in which clinicians are diagnosing small volume recurrent/persistent disease in lymph nodes of the neck. The effect of nodal recurrence/persistence on prognosis and survival is unclear, especially when it is in the form of small volume disease. Nonetheless, identification of recurrent/persistent disease requires critical thinking as to what, if any, intervention should be performed to control the disease while minimizing morbidity. This presentation discusses the preoperative and technical considerations in reoperative surgery for recurrent/persistent WDTC within the central and/or lateral necks.
Preoperative evaluation
When evaluating a patient in the reoperative setting for recurrent/persistent WDTC, a thorough preoperative evaluation is warranted to minimize the increased operative risks and, most importantly, the need for further revision surgeries. A detailed history and physical examination should be performed. It is imperative to review the previous operative reports to determine the extent of surgery performed at the initial operation. The pathology report and/or slides can provide further information regarding the extent of disease, status of the surgical margins, and integrity of the parathyroid glands. In addition, as part of the history and physical examination, it is important to ascertain if there were any associated complications with the previous surgeries. A detailed cranial nerve assessment should be performed including an analysis of vocal fold function before any reoperative surgery in the central neck. Laboratory testing should include a serum calcium level and, if low or the patient is requiring calcium supplementation, obtaining an intact parathyroid hormone (PTH) level should be considered.
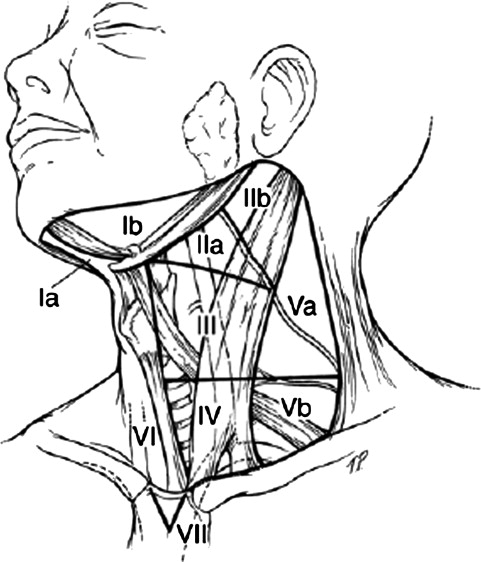
The cornerstone of postoperative surveillance for these patients is high-resolution ultrasonography of the thyroid bed and lateral neck. Ultrasound can help localize an area suspicious for recurrent/persistent disease and image-guided FNA biopsy can be used to confirm the presence of malignancy. It is important to have a clear understanding of where the disease is located as it relates to vital structures in the neck. The American Head and Neck Society has defined the compartments of the neck and this designation should be used by all practitioners so that disease localization can be clearly communicated ( Fig. 1 ). In the setting of recurrent disease in a previously operated lateral neck, a computed tomography (CT) scan of the neck with intravenous contrast can often be useful in delineating compartments that were not addressed at the time of the initial lateral neck dissection. The presence of fatty tissue harboring lymph nodes can easily be visualized in axial cuts of the CT scan; whereas a lack of a plane between the great vessels and the sternocleidomastoid muscle can suggest previous dissection in that area ( Fig. 2 ). However, before obtaining a CT scan, discussions with the endocrinologist are encouraged to ensure that this study would not delay postsurgical adjuvant radioactive iodine (RAI) treatment. An alternative study that can be used to delineate areas of previous dissection in the lateral neck but would not interfere with RAI therapy is a magnetic resonance imaging (MRI) scan with gadolinium. However, the costs associated with an MRI scan need to be considered in the context of whether the patient is a candidate for further RAI treatment.

Patterns of recurrence in the neck
Metastasis to the cervical lymph nodes is common in the tumor progression of papillary thyroid cancer (PTC) and is reported to occur in 20% to 50% of patients. Micrometastases occur at an even higher rate with a study reporting involvement in up to 90% of pathologically examined nodes. These high rates of nodal metastases may contribute to the observed persistence and recurrence rates of PTC. It has been reported that 5% to 20% of patients treated with total thyroidectomy develop palpable local recurrence within 10 years. Such recurrences have been reported to localize to the cervical lymph nodes in 60% to 75% of cases with the central compartment of the neck being the most frequently involved site. Cervical lymph node involvement has been associated with an increase in overall mortality in select patient populations. High-risk patient groups include patients older than 50 years of age with lymph node metastases greater than 3 cm in size. Patients with large nodal metastases have been shown to have increased incidence of local recurrence in the neck with involvement of the surrounding soft tissues of the neck including the carotid artery. At the time of primary surgery for WDTC, prophylactic node dissection is controversial; however, clinically positive lymph nodes should be systematically cleared to minimize the recurrence rates and need for reoperation. Reports in the literature suggest that comprehensive compartmental resection of the central or lateral neck in the setting of clinically positive lymph nodes can result in better survival and lower recurrence rates.
For recurrent/persistent WDTC cancer, an important element to achieving a successful surgical outcome is to have a systematic approach to the neck, both in surgical technique and extent of lymph node dissection within a defined compartment of the neck. Several studies have shown that for locally recurrent PTC a systematic neck dissection is recommended over simple local resection of recurrent tumors. Patients were reported to have a better prognosis after reoperation than those who underwent dissection of local lymph nodes or berry picking. In addition, several studies have demonstrated that patients who develop recurrent tumors within previously dissected areas have a worse outcome than those patients who develop recurrence outside the initial areas of dissection.
Although the pattern of cervical lymph node metastases at the time of the initial diagnosis of PTC has been described, little is known about the pattern of cervical nodal recurrence in the lateral neck and, subsequently, the extent of surgical intervention required.
Lee and colleagues reported that in the lateral neck, recurrences most frequently occurred in level IV (73.4%), followed by level III (13.3%), and level II (13.3%) and 80% of cases were found ipsilateral to the primary tumor.
Roh and colleagues evaluated the pattern of cervical nodal recurrence by performing a systematic nodal dissection of the ipsilateral central compartment as well as the lateral neck in 22 patients with recurrent/persistent PTC in the lateral neck. They reported that recurrences were common after incomplete resection of the thyroid gland with local recurrence in the remnant thyroid tissue and/or bed in patients who previously underwent partial resection of the gland. Pathologic examination of the removed lymph nodes demonstrated a high incidence (86%) of involved central nodes in patients with lateral nodal neck recurrence. Within the central compartment, the pretracheal and ipsilateral paratracheal sites were commonly involved, whereas, within the lateral compartment, the ipsilateral jugular nodes (levels II, III, and IV) were commonly involved. In contrast, the posterior triangle (level V) and contralateral lateral neck were rarely involved, and skip lesions involving the lateral but not the central lymph nodes were also rare. Because this pattern of nodal recurrence is similar to the pattern of lymph node metastases reported for incidental PTCs, it has been suggested that the lesions may have been present at the time of the initial presentation rather than presenting through altered lymphatic drainage established after the initial surgery to remove the thyroid gland.
Farrag and colleagues evaluated 53 patients with PTC who had undergone therapeutic lateral neck dissection, and 43 of these patients had recurrent/persistent disease. They found that levels IIA, III, and IV were most commonly involved with recurrent/persistent disease. Level IIB was found to harbor disease in less than 10% of patients; however, if level IIA contained metastatic lymph nodes, 100% of patients also harbored disease in level IIB. Therefore, they recommended elective dissection of level IIB only when level IIA is involved based on FNA confirmation or gross involvement intraoperatively. Level VB lymph nodes along the course of the transverse cervical vessels or adjacent to the clavicle were involved in 16 of 40 neck dissection specimens whereas level VA was involved in 0% of specimens. Based on these findings, routine dissection of level VA was not warranted; however, dissection of Level VB should be strongly considered.
Therefore, we can conclude that a reoperative lateral neck dissection should attempt to clear levels II, III, IV, and VB if this was not addressed at a previous surgery. Resection of the recurrent nodal mass alone may be sufficient in those levels of the neck that have undergone previous extensive resection. It is our contention that this formal compartmental approach to clinically positive lymph nodes in the primary or reoperative setting will help to reduce the need for further surgeries.
Patterns of recurrence in the neck
Metastasis to the cervical lymph nodes is common in the tumor progression of papillary thyroid cancer (PTC) and is reported to occur in 20% to 50% of patients. Micrometastases occur at an even higher rate with a study reporting involvement in up to 90% of pathologically examined nodes. These high rates of nodal metastases may contribute to the observed persistence and recurrence rates of PTC. It has been reported that 5% to 20% of patients treated with total thyroidectomy develop palpable local recurrence within 10 years. Such recurrences have been reported to localize to the cervical lymph nodes in 60% to 75% of cases with the central compartment of the neck being the most frequently involved site. Cervical lymph node involvement has been associated with an increase in overall mortality in select patient populations. High-risk patient groups include patients older than 50 years of age with lymph node metastases greater than 3 cm in size. Patients with large nodal metastases have been shown to have increased incidence of local recurrence in the neck with involvement of the surrounding soft tissues of the neck including the carotid artery. At the time of primary surgery for WDTC, prophylactic node dissection is controversial; however, clinically positive lymph nodes should be systematically cleared to minimize the recurrence rates and need for reoperation. Reports in the literature suggest that comprehensive compartmental resection of the central or lateral neck in the setting of clinically positive lymph nodes can result in better survival and lower recurrence rates.
For recurrent/persistent WDTC cancer, an important element to achieving a successful surgical outcome is to have a systematic approach to the neck, both in surgical technique and extent of lymph node dissection within a defined compartment of the neck. Several studies have shown that for locally recurrent PTC a systematic neck dissection is recommended over simple local resection of recurrent tumors. Patients were reported to have a better prognosis after reoperation than those who underwent dissection of local lymph nodes or berry picking. In addition, several studies have demonstrated that patients who develop recurrent tumors within previously dissected areas have a worse outcome than those patients who develop recurrence outside the initial areas of dissection.
Although the pattern of cervical lymph node metastases at the time of the initial diagnosis of PTC has been described, little is known about the pattern of cervical nodal recurrence in the lateral neck and, subsequently, the extent of surgical intervention required.
Lee and colleagues reported that in the lateral neck, recurrences most frequently occurred in level IV (73.4%), followed by level III (13.3%), and level II (13.3%) and 80% of cases were found ipsilateral to the primary tumor.
Roh and colleagues evaluated the pattern of cervical nodal recurrence by performing a systematic nodal dissection of the ipsilateral central compartment as well as the lateral neck in 22 patients with recurrent/persistent PTC in the lateral neck. They reported that recurrences were common after incomplete resection of the thyroid gland with local recurrence in the remnant thyroid tissue and/or bed in patients who previously underwent partial resection of the gland. Pathologic examination of the removed lymph nodes demonstrated a high incidence (86%) of involved central nodes in patients with lateral nodal neck recurrence. Within the central compartment, the pretracheal and ipsilateral paratracheal sites were commonly involved, whereas, within the lateral compartment, the ipsilateral jugular nodes (levels II, III, and IV) were commonly involved. In contrast, the posterior triangle (level V) and contralateral lateral neck were rarely involved, and skip lesions involving the lateral but not the central lymph nodes were also rare. Because this pattern of nodal recurrence is similar to the pattern of lymph node metastases reported for incidental PTCs, it has been suggested that the lesions may have been present at the time of the initial presentation rather than presenting through altered lymphatic drainage established after the initial surgery to remove the thyroid gland.
Farrag and colleagues evaluated 53 patients with PTC who had undergone therapeutic lateral neck dissection, and 43 of these patients had recurrent/persistent disease. They found that levels IIA, III, and IV were most commonly involved with recurrent/persistent disease. Level IIB was found to harbor disease in less than 10% of patients; however, if level IIA contained metastatic lymph nodes, 100% of patients also harbored disease in level IIB. Therefore, they recommended elective dissection of level IIB only when level IIA is involved based on FNA confirmation or gross involvement intraoperatively. Level VB lymph nodes along the course of the transverse cervical vessels or adjacent to the clavicle were involved in 16 of 40 neck dissection specimens whereas level VA was involved in 0% of specimens. Based on these findings, routine dissection of level VA was not warranted; however, dissection of Level VB should be strongly considered.
Therefore, we can conclude that a reoperative lateral neck dissection should attempt to clear levels II, III, IV, and VB if this was not addressed at a previous surgery. Resection of the recurrent nodal mass alone may be sufficient in those levels of the neck that have undergone previous extensive resection. It is our contention that this formal compartmental approach to clinically positive lymph nodes in the primary or reoperative setting will help to reduce the need for further surgeries.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


