Purpose
To investigate the correlation between choroidal and retinal lesions in eyes with acute Vogt-Koyanagi-Harada disease (VKH) using optical coherence tomography (OCT) by using a new parameter, retinal pigment epithelium (RPE) undulation index, which quantitatively describes choroidal deformations.
Design
Retrospective, observational, cross-sectional study.
Methods
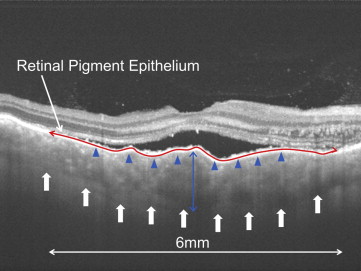
Spectral-domain OCT (SD OCT) and swept-source OCT images from a consecutive series of 42 eyes in 22 patients with acute VKH who underwent steroid therapy and 20 healthy eyes in 20 volunteers were analyzed retrospectively. Correlations between best-corrected visual acuity (BCVA), axial length change, and OCT parameters were examined. The RPE undulation index was defined as RPE line length to the total scan length ratio on a foveal-centered scan in the SD OCT image.
Results
Eyes with acute VKH showed increased RPE undulation index, choroidal thickness, and retinal thickness compared to normal subjects, which were reduced following steroidal treatment ( P < .0001, P = .0003, and P < .0001, respectively). RPE undulation index was related to choroidal thickness ( r = 0.624, P = .0043), retinal thickness ( r = 0.483, P = .0028), and BCVA ( r = 0.588, P = .0002). Meanwhile, no statistically significant relationship was observed between choroidal thickness and retinal thickness. Axial length changes were significantly correlated with both choroidal thickness ( r = 0.842, P < .0001) and RPE undulation index ( r = 0.600, P = .0139).
Conclusions
This study demonstrated that the choroid was diffusely undulated and bulged inward in eyes with acute VKH. Correlations between RPE undulation index and choroid morphology, retinal thickness, and poor BCVA suggest that choroidal folding, quantified by RPE undulation index, is useful in assessing VKH disease severity.
Vogt-Koyanagi-Harada disease (VKH) is characterized by diffuse granulomatous uveitis and is the second-leading cause of uveitis in Japan, after Beh ç et syndrome. Inflammatory manifestations of VKH are thought to result from an autoimmune reaction to melanocytes, but the exact mechanism of disease development remains unknown.
One useful tool in studying VKH is optical coherence tomography (OCT), which facilitates visualization of retinal and choroidal structures. With recent advances in imaging technology, OCT can be used to diagnose ocular diseases, including VKH, and evaluate efficacy of prescribed ophthalmologic therapies. Increases in retinal scan speed (ie, advancement from time-domain OCT to spectral-domain OCT [SD OCT]) and improvements in image processing techniques (eg, speckle noise reduction with multiple-aligned OCT scans) have been particularly beneficial.
The OCT has already been used to observe retinal and choroidal structures in eyes with acute VKH. Serous retinal detachment and subretinal cystoid spaces have been observed. Swept-source OCT (SS OCT), which uses a 1050-nm tunable laser and allows 3-dimensional (3D) high-penetration imaging of deep fundus tissue, has enabled imaging of the deep choroidal structures. This is possible because SS OCT uses a deeper penetrating light source than SD OCT, so light can penetrate through the retinal pigment epithelium (RPE) to the choroid.
Enhanced depth imaging OCT (EDI-OCT) recently revealed that patients with acute VKH disease have a markedly thickened choroid. It also revealed that treatment decreases choroidal thickness, with significant differences between the acute disease stage and remission. These observations are in agreement with pathologic studies, which have shown that, in eyes with VKH, the choroid thickens from lymphocytic infiltration, choroidal melanocytes disappear because of inflammation, and nongranulomatous lymphocytes infiltrate the choroid during the convalescent stage. The SD OCT and SS OCT techniques have also revealed that high-dose corticosteroid therapy decreases choroidal thickness in eyes with VKH. In these eyes, choroidal folds appear as choroidal lesions, which are more easily detected with OCT than with angiography.
Given that the sclera is more rigid than the retina, we hypothesized that VKH causes the choroid to thicken and deform toward the retina. This would subsequently result in added mechanical stress to the retina, which may eventually lead to retinal lesion development. To the best of our knowledge, there have been no previous attempts to correlate choroidal and retinal lesions in eyes with VKH. Thus, in this study we proposed a new parameter, the RPE undulation index, which reflects the severity of choroidal deformation. Relationships between RPE undulation index, choroidal thickness, and retinal thickness were explored in patients with VKH using SS OCT and SD OCT.
Methods
Subjects and Ophthalmic Examinations
This was a retrospective, observational study. Study conduct adhered to the tenets of the Declaration of Helsinki and this retrospective review of existing patient data was approved by the Institutional Review Board at Kyoto University Graduate School of Medicine. We retrospectively examined 42 eyes with VKH from 22 patients (mean age ± standard deviation, 46.0 ± 16.9 years; range, 13–76 years) who visited Kyoto University Hospital between Novenber 29, 2007 and April 8, 2013. Eyes with ocular diseases that might have interfered with functional and/or structural results (eg, retinal detachment, trauma, diabetic retinopathy) were excluded from analyses. At the initial visit, all patients underwent comprehensive ophthalmologic evaluations. This included standardized refraction and measurement of best-corrected visual acuity (BCVA) using a Landolt ring, slit-lamp biomicroscopy, OCT imaging, and color fundus photography. Following the VKH diagnosis, patients were treated with intravenous methylprednisolone (200 mg/day for 3 days, followed by 150 mg/day for 3 days, followed by 100 mg/day for 3 days), followed by a tapering oral prednisolone regimen (starting dose of 50 mg/day). Treatment effects were monitored with weekly SD OCT imaging until serous retinal detachment resolution. Data from 20 healthy eyes from 20 volunteers (mean age ± standard deviation, 49.2 ± 22.4 years; range, 20–78 years) were also retrospectively collected from our database as a control data set.
Quantitative Analysis of Retinal Imaging
The Spectralis OCT system (Heidelberg Engineering, Heidelberg, Germany) was used to obtain SD OCT images of all included eyes. Retinal scans were performed at 30 degrees, along the horizontal and vertical planes through the foveal center. The Spectralis OCT has built-in software to calculate retinal thickness, which was defined as the distance between the vitreoretinal interface and Bruch membrane. This feature was used to measure average retinal thickness in a 6-mm-diameter circular area that was centered on the fovea. Measurements were automatically made on horizontal foveal scan images. Scans that had any B-scans with algorithm failures (eg, automated boundary lines inaccurately drawn) were manually corrected.
Quantitative Analysis of Choroid Images
Choroidal thickness measurements
The SS OCT (Topcon 3D-2000 OCT; Topcon Corporation, Tokyo, Japan) was used to measure choroidal thickness before steroid therapy and after complete resolution of serous retinal detachment. Choroidal thickness was defined as the vertical distance between the RPE line and the hyper-reflective line behind the large choroidal vessel layers (ie, subfoveal choroidal-scleral interface, Figure 1 ). It is important to note that choroidal thickness was evaluated underneath the fovea rather than at the thickest point. When the choroid was so thick that the choroidal-scleral interface was not visible in VKH patients (n = 2 eyes), a thickness value of 1000 μm was assigned.
Choroidal fold quantification
Choroidal thickening and choroidal folds were measured as indicators of inflammation. Choroidal folds, imaged on foveal SD OCT scans, were defined as bumpy RPE undulation. The RPE undulation index was used to calculate the degree of deformation, as follows:
RPE undulation index = ( L h + L v ) / 12 000
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


