Chapter 6
REHABILITATION OF PATIENTS WITH OCULAR TRAUMA

Because the visual system alone provides more input to the brain than all other senses combined, vision loss can have a devastating impact on people’s lives.
PEARL… In our daily medical practice, we usually narrow our focus on acute care, to minimize the impact of a disease on an organ or system. Trauma, however, has a much greater impact; for example, eye injury affects the quality of life of the individual far beyond the globe.
Health care promotes health: a condition of optimal physical, mental, and social well-being (WHO definition).With a focus different from that of acute care, rehabilitation medicine, irrespective of the organ system involved, tries to reduce the functional impact of the impairment so that the individual can maintain:
• independence;
• productive activity; and
• life satisfaction.
REHABILITATION GOALS
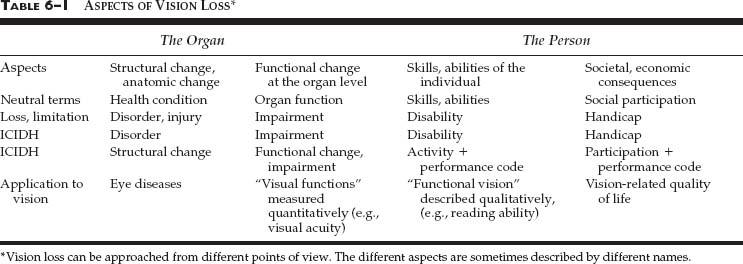
Rehabilitation is best approached (see Table 6–1) via the following four terms1,a.
1. Disorder (describing aspects of the organ’s condition, i.e., anatomic/structural changes).
3. Disability (describing aspects of the person’s condition, i.e., generic skills and abilities).
4. Handicap (describing aspects of the person’s condition, pointing to the social and economic consequences of a loss of abilities).
PEARL… In colloquial use, persons with severe vision loss are often called “blind.” This term is inappropriate as most people have residual vision.
Improving participation is the ultimate goal of all medical and social interventions. There are obvious links between them: a disorder may cause an impairment, which may cause a loss of abilities, which may cause a lack of participation. Each of these links may be aggravating or compensating, and the very possibility of rehabilitation depends on this flexibility. For example:
• medical/surgical interventions can reduce disorder- related impairment;
• assistive devices may improve abilities in the presence of a given impairment;
• changes in the human and physical environment may increase participation regardless of reduced abilities.
The art of rehabilitation is to manipulate each of these links so that a given disorder results in the least possible loss of participation.
TEAMWORK
Figure 6–1 illustrates that different interventions, provided by different professionals, are needed at different points in the chain. Because ophthalmologists are early participants, it is their responsibility to call upon other team members appropriately.
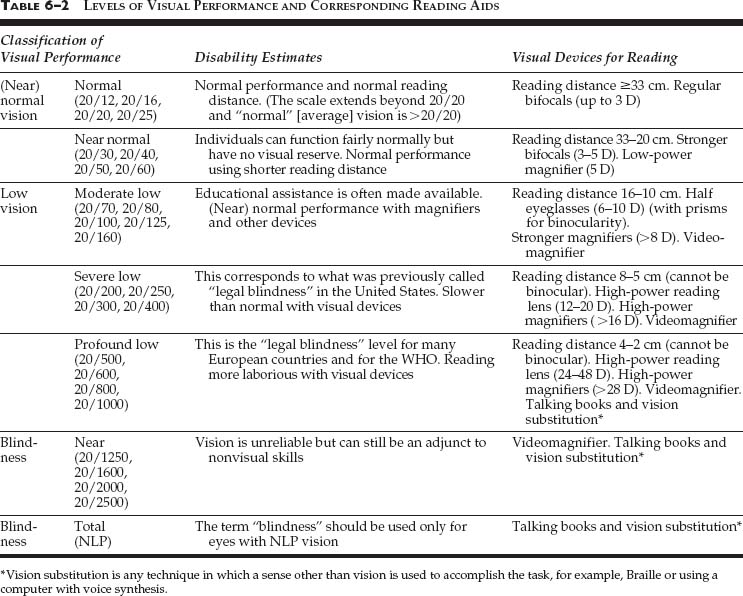
RANGES OF VISION LOSS
The simplest scale, adopted by the WHO in 1974, has three ranges:
1. normal vision (normal and near-normal);
2. low vision (moderate, severe, profound); and
3. blindness (near blindness, total blindness).
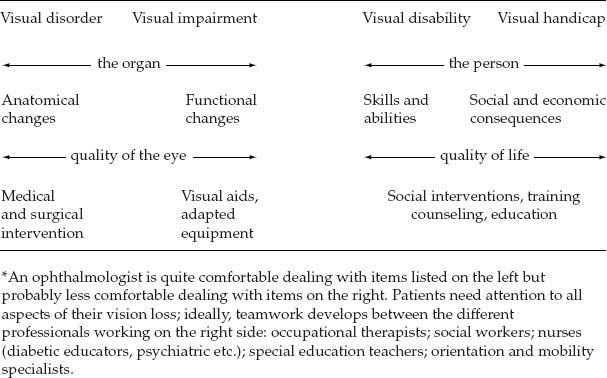
FIGURE 6–1 Modes of intervention. (From International Classification of Impairments, Activities and Participation [ICIDH-2-Beta-2]. Geneva: World Health Organization, under development. Available at www.who.ch/icidh.)
By acknowledging the “low-vision” range,b this scale has abandoned the old dichotomy between those who are considered “legally sighted” and those who are considered “legally blind.”c