A growing number of children with severe-to-profound hearing loss are receiving cochlear implants. This article provides information about the various educational and rehabilitation options for these children, emphasizing the need for a collaborative approach to rehabilitation planning and implementation. Decisions about such options should be individualized and are informed by several factors including age at implantation and family expectations and desires. A review of legislation affecting the education of children with hearing loss is also provided.
Cochlear implants improve numerous outcomes for children with hearing loss. They make spoken language a viable communication option for those with severe-to-profound losses, improve speech perception and speech production skills, and contribute to improved reading outcomes for school-aged students. Moreover, the use of cochlear implants increases the likelihood that children with hearing loss can be included in general education settings. These findings are encouraging; however, the device is rarely the sole contributor to these positive outcomes. Systematic rehabilitation and educational programming are necessary for cochlear implant recipients to reach their full potential.
This article focuses on rehabilitation and educational considerations for children with cochlear implants. Although distinctly different, the goals of rehabilitation and education overlap considerably in good practice. The term rehabilitation is typically used to refer to an individualized model of therapy, such as one-on-one training with a speech-language pathologist or auditory-verbal therapist 1
1 An auditory-verbal therapist is a speech-language pathologist, audiologist, or teacher of the deaf who specializes in teaching children with hearing loss to develop spoken language through the development of audition. The auditory-verbal therapist also guides and coaches the family. The Alexander Graham Bell Academy for Listening and Spoken Language oversees the certification of auditory-verbal therapists.
; education typically refers to learning facilitated by a teacher in a school-based environment. Children with cochlear implants benefit from the intentional collaboration of these 2 practices. For example, teachers should integrate speech and language goals into academic lessons and speech-language pathologists should integrate academic content into speech and language activities. This article uses the terms interchangeably as a reminder of their ideal interconnectedness.Overview of deaf education
The roots of deaf education date back to the early sixteenth century in Western Europe. However, it was not until the nineteenth century that deaf education came to the United States. Thomas Hopkins Gallaudet, a graduate of Yale University and an ordained minister, helped establish the first permanent school for the deaf in 1817. Now called The American School for the Deaf, the institute’s first teacher was a deaf man Gallaudet met while studying manual education methods in France. This teacher, Laurent Clerc, is credited with the development of American Sign Language (ASL) and was responsible for training many of the first teachers of the deaf. Fifty years later, oral education was introduced. These programs were designed for children who were adventitiously, and postlingually, deafened. Shortly after World War II, transistors were invented, which greatly reduced the size of hearing aids. This miniaturization of hearing aids permitted more practical use of the devices, especially in children. As amplification devices became more sophisticated, oral communication expanded to children who were congenitally deaf. Educational recommendations were subsequently based on degree of hearing loss. Children with adequate residual hearing were considered candidates for the oral approach; manual education programs were recommended for children with limited residual hearing. However, approval of the use of cochlear implants in children in the 1990s expanded the option of oral communication to those with profound hearing loss. Today, children with diverse types and degrees of hearing loss are served by a wide variety of educational approaches.
Historically, the educational program chosen for children with hearing loss has been linked with their communication modality. Although the dichotomy of spoken (oral) versus signed (manual) language is predominant, there are a variety of communication modalities that span across a continuum:
- 1.
ASL. ASL is often referred to as the language of the Deaf community (ie, people who affiliate themselves with deaf culture). It is a rich and vibrant language, complete with unique syntactical and morphologic elements that are distinct from English. Deaf children of deaf parents, who receive exposure to ASL from infancy, develop linguistic competence comparable with hearing children of hearing parents, albeit not in English. ASL is used in residential and day schools for the deaf, as well as in classrooms located in both public and private institutions.
- 2.
Total communication (TC). TC refers to a diverse group of communication options that combines manual signs with spoken language. Sign systems, such as Signing Exact English (SEE) and pidgin signs, are typically used because of their compatibility with English word structure. This approach also includes the bilingual-bicultural method, which treats English instruction as a second language for students whose first language is ASL.
- 3.
Auditory/oral. Oral communication options rely on amplification and use of residual hearing to develop audition and spoken language. This modality is used in both public and private schools, including special schools designed for children with hearing loss. Cued speech, a visual system used to improve speech reading, is also in this category.
Although these 3 categories simplify the variety of communication types and educational programming options available to children with hearing loss, they provide a framework for the common approaches that have resulted from the selection of communication modality. These categories are not mutually exclusive; children with hearing loss might participate in any or all of these programs at various times throughout their education.
Approximately 90% of children with hearing loss are born to parents who have normal hearing, so the number of parents choosing oral methods for their children’s education is increasing. From the 1999 to 2000 until the 2007 to 2008 school years, students relying exclusively on spoken language as their primary method of instruction increased from 44% to 52%. Moreover, 87% of children with hearing loss are using some degree of spoken language in educational settings.
Cochlear implants have allowed the education of students with hearing loss to follow the national trend toward educating students with disabilities alongside their typically developing peers. Instead of attending residential schools, children with hearing loss are increasingly being educated in their neighborhood schools. During the 2007 to 2008 school year, approximately 60% of students with hearing loss were included in general education classrooms. Regardless of communication modality, early identification and intervention for hearing loss facilitates the development of language skills that lead to increased participation in general education classrooms.
Educational Legislation
The education of students with hearing loss is governed by federal legislation. In 1975, Public Law 94-142, the Education of All Handicapped Children Act, radically changed the concept of special education. The primary provisions mandated that students with disabilities receive a free, appropriate, public education; be educated in the least restrictive environment; and receive an Individualized Education Program (IEP). In 1990, this law was amended by the Individuals with Disabilities Education Act (IDEA), which was divided into 4 parts :
- A.
General provisions
- B.
Special education services for children and youth
- C.
Early intervention services for infants and toddlers
- D.
National activities for improving the education of students with disabilities.
Parts B and C relate directly to educating students with hearing loss.
Part C of IDEA covers infants and toddlers from birth until age 3 years. The provisions are designed to improve long-term outcomes for children with disabilities through early intervention. The focus of early intervention is to empower families to meet their children’s developmental needs. Several professionals are involved in this process, including audiologists who assess the child’s hearing, otologists who assess the cause of the hearing loss, and early interventionists who provide family-centered therapy. Similar to an IEP, an Individualized Family Service Plan (IFSP) is a legal document developed to guide the rehabilitation process for children and their families. The provisions in part C, along with the rest of IDEA, enable the development of effective educational plans for children with cochlear implants.
Part B of IDEA addresses school-aged children and youth (aged 3–21 years) and provides specific guidelines for educational services. Before the mandate of free, appropriate, public education, children with hearing loss, as well as those with other 1 exceptionalities, were systematically denied access to individualized rehabilitation. The law does not guarantee services to every child with a disability, or to every child with a hearing loss. Students must show a need, resulting from the disability, for specialized educational programming. Although disagreements exist about what constitutes appropriate services, students with hearing loss often have delayed language skills that negatively affect their educational performance, thus qualifying them for services under IDEA.
When a child qualifies for services, the educational team develops an IEP based on the student’s current functioning level. The team is typically composed of a special educator, a general educator, a local education agency representative, and the parents/guardians of the child. Other members might include school administrators, related service providers (eg, speech-language pathologists, audiologists, occupational therapists, psychologists), and the students themselves. The IEP team makes numerous educational decisions, including which services are needed, how often and in which settings the services will be provided, and how progress on selected goals will be evaluated. The IEP is updated at least annually and serves as a unique blueprint for each child’s specific educational needs.
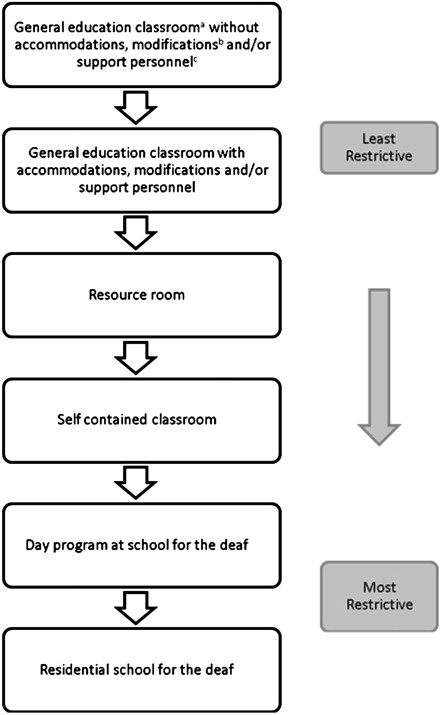
An important task for the IEP team is to determine the least restrictive environment in which rehabilitation should occur. A continuum of possible placements is shown in Fig. 1 . The specific needs of each individual student also need to be considered. These needs include academic supports (eg, teacher of the deaf, interpreters, hearing technology) as well as opportunities for socialization. The child’s environment should be continuously evaluated to reflect the child’s development and to achieve the family’s desired outcome.
Factors Influencing Rehabilitation and Education
Several studies have documented the variability of outcomes for children with cochlear implants. A cochlear implant, even when provided at a young age, does not guarantee the acquisition of age-appropriate listening and spoken language skills, general educational placement, or successful academic and social outcomes. Some factors that influence outcomes are age of implantation, participation in early intervention, and presence of additional disabilities. Evidence of the impact of underlying neurocognitive processes is also emerging.
A rehabilitation plan developed through collaboration among professionals is necessary to meet the child’s needs and facilitate desired outcomes. Each of the professionals involved (the otologist, the audiologist, the speech-language pathologist, and the teacher of the deaf) makes a distinct and essential contribution to the rehabilitation process. For example, the teacher of the deaf might report a child’s difficulty with auditory discrimination in noise. The audiologist can then create a separate speech-in-noise program in the implant for use in adverse listening conditions. Purposeful collaboration at different stages of rehabilitation, including candidacy decisions and periodic evaluation of performance ( Table 1 ), identifies changing needs expediently, allows for ongoing adaptation of the rehabilitation plan, and helps maintain realistic expectations for families.
| Steps in the Rehabilitation Process | Parent | Otologist | Audiologist | Speech-Language Pathologist | Teacher of the Deaf | General Education Teacher | |
|---|---|---|---|---|---|---|---|
| 1. | Determine candidacy for cochlear implantation | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| 2. | Assess physiologic structures/function for implant compatibility | — | ✓ | ✓ | — | — | — |
| 3. | Implant the device and monitor the internal device function in the operating room | — | ✓ | ✓ | — | — | — |
| 4. | Program the implant for maximum auditory access | — | — | ✓ | — | — | — |
| 5. | Assist with maintenance and troubleshooting of cochlear implant | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| 6. | Develop age-appropriate speech, language, and auditory skills | ✓ | — | ✓ | ✓ | ✓ | ✓ |
| 7. | Develop age-appropriate academic and social skills | ✓ | — | — | ✓ | ✓ | ✓ |
| 8. | Evaluate and monitor progress | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| 9. | Develop goals and objectives for Individualized Education Plan/IFSP | ✓ | — | ✓ | ✓ | ✓ | ✓ |
| 10. | Facilitate opportunities for meaningful interaction with normal-hearing peers | ✓ | — | — | ✓ | ✓ | ✓ |
| 11. | Educate parents and other professionals about cochlear implants | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
The rehabilitation plan should take into account the various mitigating factors related to:
- 1.
The child receiving the implant
- 2.
The family of the recipient
- 3.
The rehabilitation supports
Reed and colleagues identified the unique contributions of each of these factors to the academic success of children with hearing loss. Each is described later in relation to the rehabilitation of children with cochlear implants.
Child Receiving the Implant
Rehabilitation teams consider the individual characteristics of the child, especially the present level of performance on academic, speech-language, and auditory tasks, and the presence of additional disabilities. Input from all professionals regarding the child’s abilities before implantation is necessary to develop a plan that builds on the child’s current level of skills. For example, the rehabilitation plan for a 3-year-old with profound hearing loss who has limited auditory and language skills should be distinctly different than that for a 6-year-old who has a progressive hearing loss and age-appropriate language skills.
The presence of an additional disability adds a new dimension to the rehabilitation plan. The unique impact of the additional disability on overall development will likely require the team to develop a plan and establish benchmarks for measuring progress that are different from the ones used for children with hearing loss only.
Family Involvement and Expectations
Discussion regarding the parents’ desired outcomes after implantation is essential for setting realistic expectations, planning rehabilitation, and recommending educational options. For example, the rehabilitation plan for a 12-month-old whose parents want him to develop listening and spoken language and go to a mainstream school alongside his hearing peers is vastly different than that for a 12-month-old whose parents want her to learn spoken English and ASL and be part of the deaf community.
Parental involvement and expectations are positively correlated with academic achievement. That is, children of parents who have high expectations, maintain consistent communication with the school, help with homework, and enroll their children in extracurricular activities have better academic outcomes. Educating parents to be active participants in the rehabilitation process is critical to their children’s successful use of cochlear implants. Typically, parents of children with cochlear implants are responsible for:
- •
Maintaining and troubleshooting the equipment
- •
Providing transportation to 1 or more therapies
- •
Providing academic support beyond the level typical of hearing children
- •
Facilitating opportunities for social skill development
- •
Advocating for education and rehabilitation services
- •
Educating school personnel about cochlear implants and the impact of hearing loss on development
Parents need to understand the importance of their continued involvement in the rehabilitation process and receive support from the rehabilitation team to follow through with the recommendations. The following questions should be addressed by the rehabilitation team before cochlear implantation and throughout the rehabilitation process:
- •
What is the family’s desired outcome for the child?
- •
What are the recommendations for rehabilitation and education?
- •
What types of support are available through the implant center, local early intervention system, and school system?
- •
What resources (physical, social, financial) does the family have to follow these recommendations?
- •
What is the role of the family in the rehabilitation process?
As noted previously, there is wide variation in outcomes for children who receive cochlear implants. It is rare, but not impossible, for some children to receive minimal or no benefit from the implant and the rehabilitation process. However, 87% of parents report wanting their children to use spoken language to communicate after receiving an implant. Although all the factors influencing outcome variability are not yet fully understood, professionals have a responsibility to provide parents with appropriate and adequate information about all potential outcomes.
Rehabilitation Supports
Achievement of desired outcomes requires a rehabilitation plan that meets the needs of the child and facilitates development of auditory, language (spoken and/or signed), and academic skills. At a minimum, supports in the following areas should be considered as necessary supplements to educational intervention:
Audiological management
Access to an implant center is essential to ensure the maintenance of the cochlear implant. Being far away from an implant center is stressful for parents and can have a negative impact on the language and academic outcomes of children. Experience suggests that children who have difficulty accessing the services of an implant center might experience longer periods of time between mapping sessions, spend more days waiting for equipment to be replaced or serviced, and lose valuable listening time as a result of damaged or malfunctioning equipment. Although all families cannot be expected to move their homes to be close to implant centers, it is becoming increasingly common for cochlear implant programming and troubleshooting to be available via telehealth options. Implant manufacturers and cochlear implant teams should be able to advise families of such options.
Speech and language therapy
When the desired outcome of cochlear implantation is to develop listening and spoken language skills, intensive speech and language therapy is necessary. Although services differ based on each child’s current level of performance, it is recommended that children receive auditory-based therapy after implantation to maximize benefit from the cochlear implant. The speech-language pathologist focuses on developing listening skills to facilitate language acquisition. The teacher of the deaf complements the speech-language pathologists by focusing on language through academic development. However, few speech-language pathologists are currently trained to work with children with hearing loss who are developing listening and spoken language. Thus, the rehabilitation team should collaborate with the speech-language pathologist and provide information and resources.
Academic services
Teachers of the deaf are trained to develop language skills (spoken or signed) to support academic instruction and social development. Some teachers of the deaf work at one specific school; others are itinerant teachers who serve numerous students at multiple locations. Because the inclusion of children with hearing loss in general education classrooms is increasing, teachers of the deaf are often responsible for collaborating with general education teachers. A factor that contributes to academic success is the willingness of general education teachers to support the child with hearing loss, but maintain appropriate academic expectations. That is, a general education teacher should provide the tools for learning (eg, study guides, modified tests) but expect children to participate to the best of their abilities.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


