Fig. 12.1
The glottis: anterior and posterior glottis
Clinically, more attention is usually paid to the anterior glottis because most lesions that cause dysphonia occur in this region. Therefore, regenerative treatment has chiefly been considered for the anterior glottis, the vocal fold.
12.1.2 Architecture of the Vocal Fold Mucosa
The vocal fold lies between the anterior commissure and the vocal process of the arytenoid cartilages. The vocal fold has unique vibratory properties that are not seen in any other part of the body. These unique properties are supported by its histological architecture, and disruption of the normal architecture causes severe dysphonia that is difficult to treat.
The well-defined layer structure of the vocal fold has been well characterized and consists of the epithelium, lamina propria, and muscle [1, 2] (Fig. 12.2). The epithelium covering the free edge of the vocal fold is a squamous epithelium, while ciliated columnar epithelium covers the supra- and subglottic mucosa. The lamina propria is divided into three layers: the superficial, intermediate, and deep layers. The superficial layer is composed of sparse fibrous tissue and abundant amorphous substances, which makes it more pliable than the other layers. This layer is called “Reinke’s space,” and it is the main site where mucosal vibration occurs during phonation. Most benign and malignant pathologies affect this region resulting in voice problems. The intermediate layer chiefly consists of elastic fibers, while the deep layer primarily consists of collagenous fibers. These two layers form the vocal ligament, which is connected to the conus elasticus inferiorly and to the anterior commissure tendon anteriorly. The vocalis muscle lies beneath the vocal ligament and forms the main body of the vocal fold. The boundary between the deep layer of the lamina propria and the muscle is not distinct because some collagenous fibers from the deep layer insert into the muscle tissue.
Fig. 12.2
Layer structure of the vocal fold mucosa. The lamina propria consists of three layers: superficial, intermediate, and deep layers. SLP superficial layer of lamina propria, ILP intermediate layer of lamina propria, DLP deep layer of lamina propria, TA thyroarytenoide (By courtesy of Minoru Hirano)
The muscle is the contractile element that supplies a firm scaffold, while the vocal ligament provides a substrate of appropriate stiffness and elasticity on which the pliable superficial layer vibrates. Stiffness decreases from the muscle to the superficial layer of the lamina propria, that is, the pliability of the tissues gradually increases in the same order. This gradation of the different tissue properties is thought to be ideal for the vibratory function of the vocal fold. This concept is called the “cover body theory,” according to which the cover consists of the epithelium and the superficial layer of the lamina propria, while the body consists of the muscle; the intermediate to deep layers of the lamina propria are referred to as the transition [1, 3]. The average thickness of the lamina propria in adults is only 1 mm.
12.1.3 Basement Membrane Zone (BMZ)
The basement membrane zone forms the boundary between the epithelium and the superficial layer of the lamina propria (SLP) and plays an important role in securing this boundary. This zone is directly affected by phonotrauma and any other injuries to the vocal fold. Gray and colleagues have extensively investigated the architecture of the BMZ and its alteration by benign pathology [4, 5]. The basement membrane consists mainly of laminin and type IV collagen. Gray et al. found that type VII collagen fibers connect the basement membrane with the SLP, firmly maintaining the relationship between them; these are called “anchoring fibers.” Sato et al. also found type III collagen fibers, called “reticular fibers,” in the SLP [6]. The reticular fibers are thin fibrils that may contribute to maintaining the architecture of the SLP. The collagen network consisting of collagen type IV, VII, and III in the BMZ and SLP is thought to be important for maintaining the structure of the “cover.”
12.1.4 Extracellular Matrix (ECM) of the Superficial Layer of the Lamina Propria
The SLP primarily vibrates in sync with the epithelium forming a traveling wave. After injury to the vocal fold mucosa, the SLP is the most important and main site of wound healing. The tissue properties of the SLP are defined by deposition of ECM. As mentioned above, the SLP has a low content of fibrous proteins, but is rich in a variety of interstitial proteins (proteoglycans: PGs) and glycosaminoglycans (GAGs). These molecules play a key role in determining the properties of the SLP.
One of the most important molecules is hyaluronic acid (HA). HA is a mucopolysaccharide and one of the glycosaminoglycans found in the vocal fold. It is abundant in the SLP, and is thought to be a key molecule for determining the viscoelasticity of the vocal fold mucosa [7]. In general, a higher content of HA leads to an increase in tissue viscosity [8]. Rheological studies have revealed that HA has a similar viscoelasticity to the human vocal fold mucosa [9], while removal of HA alters the stiffness and viscosity of the vocal fold [10].
12.1.5 Fibroblasts in the Lamina Propria
Fibroblasts in the lamina propria are primarily responsible for producing ECM. Two different kinds of fibroblasts have been reported: fibroblasts in Reinke’s space (SLP) and fibroblasts in the macula flava [13]. Fibroblasts are sparse in the SLP where most of these cells are oval or spindle-shaped. Hirano et al. have found only occasional intracellular organelles such as the Golgi apparatus (GA) and rough endoplasmic reticulum (rER) in fibroblasts from the SLP, indicating lower protein-producing activity by these cells.
The macula flava is located at the anterior and posterior ends of the intermediate layer of the lamina propria (ILP) (Fig. 12.3) [14]. The anterior macula flava forms an oval mass near the anterior end of the ILP and is composed of a fine mesh of elastic fibers and fibroblasts. It is connected to the anterior commissure tendon anteriorly. The posterior macula flava is situated at the posterior end of the ILP and is connected to the vocal process. The macula flava is abundant in fibroblasts, and these fibroblasts are predominantly stellate in shape (Fig. 12.4) [15]. GA and rER are prominent in these cells, suggesting active production of ECM proteins. Histological studies have demonstrated increased production of hyaluronic acid, collagen, and elastin around the fibroblasts. Based on these histological features, it has been suggested that the cells in the macula flava may contribute to the maintenance of the ECM in the lamina propria, although few studies have conducted functional analysis of these cells to support this hypothesis.
Fig. 12.3
Axial plane of the vocal fold. AMF anterior macula flava, PMF posterior macula flava, VP vocal process (By courtesy of Minoru Hirano)
Fig. 12.4
Fibroblasts in the macula flava. (a) Stellate shape. N nucleus, EF elastic fiber, CF collagenous fiber. L lipid droplet, B and C indicates the figures b and c. (b) Intracellular organelle. rER rough endoplasmic reticulum, V vesicle, M mitochondria. (c) Lipid droplet containing vitamin A (Cited with permission [15])
12.2 Alteration of the Vocal Fold
12.2.1 Vocal Fold Scar
Vocal fold scarring is a consequence of inflammation or injury to the vocal fold mucosa, which stiffens the mucosa [16] (Fig. 12.5). The scarred vocal fold has difficulty vibrating, which causes the voice to become harsh, hoarse, strained, and even aphonic. Stroboscopic examination of scarred vocal folds shows asymmetric amplitude of vibration and reduced/absent mucosal wave with glottic incompetence. To date, there has been no optimal treatment established for restoring normal properties to the scarred vocal fold.
Fig. 12.5
Vocal fold scar. Arrow indicates scar tissue with higher stiffness
Histological alterations within the SLP are the main cause of stiffening of the scarred vocal fold. Histological analysis of human scarred vocal fold tissue after cordectomy shows increased and disorganized collagen deposition forming thick bundles, decreased elastic fibers and/or hyaluronic acid (HA) in the SLP [17] (Fig. 12.6). These findings cause fibrosis of the mucosa with reduced viscoelastic property. An increase in fibronectin in scarred vocal folds is thought to contribute to the increasing stiffness of the mucosa. Several animal studies using vocal fold scar models have also revealed similar histological findings [18–20]. It is clear that restoration of this deteriorated structure is key to regenerating the vocal fold.
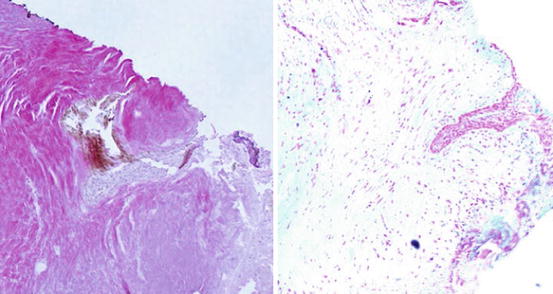
Fig. 12.6
Histology of scarred vocal fold. (Left) Elastica-von-Gieson stain (×4). The lamina propria is occupied with disorganized collagen (stain red) forming thick bundles. (Right) Alcian blue stain (×4). Few hyaluronic acid is observed
12.2.2 Vocal Fold Sulcus (Sulcus Vocalis)
Vocal fold sulcus is defined as a deformation of the vocal fold mucosa with a sulcus along the mucosa; this causes a spindle-shaped glottis with bowing of the mucosa (Fig. 12.7). The sulcus causes a decreased mucosal wave, decreased amplitude of mucosal displacement, and makes the vibration aperiodic and asymmetric. This results in the voice becoming breathy, hoarse, strained, and strangled.
Fig. 12.7
Histology of Sulcus vocalis. Sulcus (arrow) is formed at the free edge of the mucosa where the epithelium is attached to the vocal ligament (By courtesy of Minoru Hirano)
The etiology of sulcus formation is controversial [21]. It can occur congenitally or be acquired by inflammatory processes. The histology often shows that the epithelium is attached directly to the vocal ligament at the bottom of the sulcus, and the SLP is replaced with fibrotic tissue. This results in the mucosal wave being disturbed at the sulcus. Although several phonosurgical treatments have been attempted to improve voice, complete and consistent treatment of the deformed mucosa remains difficult.
12.2.3 Vocal Fold Atrophy
Atrophy of the vocal fold mucosa usually occurs during the aging process. With age, the vocal fold mucosa becomes thin and bowed, which causes reduced amplitude of the mucosal wave and glottic insufficiency. This results in the voice becoming hoarse and harsh. Histological analysis indicates increased deposition of disorganized collagen and reduced elastin/HA in the SLP, causing fibrotic changes in the mucosa [22, 23]. The treatment of aged vocal folds also remains a challenge. Voice therapy, including vocal exercise, can help in some cases, and medialization procedures have been shown to have limited effects. It is thus important to regenerate the mucosa in order to treat vocal fold atrophy.
12.3 Regenerative Medicine for the Vocal Fold
12.3.1 Regeneration Targets and Strategy
Targets of regenerative medicine for the vocal fold include the disturbed vocal fold mucosa in cases such as scarring, sulcus, and atrophy. Based on the findings described above, regeneration of the vocal fold requires multiple elements including cells and ECM. The key is to restore the normal distribution of ECM in the mucosa, which requires the modulation of cell function in the vocal fold. The targets of a regenerative approach should be the cells in the vocal fold including fibroblasts, endothelial cells, epithelial cells, muscle cells, and possibly tissue-specific stem cells. Another regenerative target is the ECM of the mucosa itself.
Tissue engineering approaches involve cells, scaffolds, and regulatory factors. One of the most potent regulatory factors is growth factors that modulate cell function in terms of proliferation, migration, and production of ECM proteins. The appropriate combination of scaffold/cell/growth factor should be more effective for regenerating the vocal fold than any factor alone.
12.3.2 Scaffolding
Scaffolding strategies aim to regenerate tissue by implanting regenerative scaffold into the target organ (Fig. 12.8). Ideal regenerative scaffolds are biocompatible and biodegradable. They should also possess properties that attract an influx of cells and growth factors from surrounding tissues. A favorable interaction between scaffold and cells will enable the formation of new healthy tissue. Since a scaffold is a foreign body, it should be absorbed over time but should be retained for a long enough period to achieve the formation of new tissues. Several types of scaffolds have been studied for use in regeneration of the vocal fold.
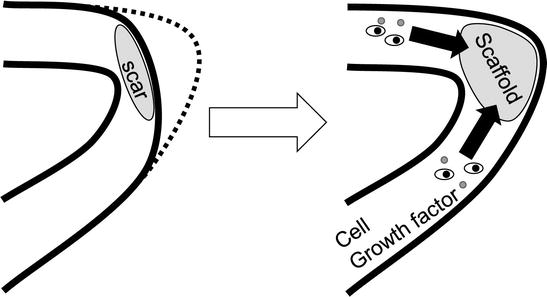
Fig. 12.8
Scheme of Scaffolding. The scar tissue is replaced with scaffold. Cells and growth factors are expected to be supplied from surrounding tissue
12.3.2.1 Collagen-Gelatin Material
We have examined the feasibility of bovine-derived atelocollagen sponge (Terdermis ®, Terumo CO., Tokyo) as a scaffold for vocal fold regeneration. To first confirm biocompatibility of the scaffold, rat mesenchymal stem cells (MSCs) were cultured on the scaffold and the cells were found to survive and proliferate well, producing fibronectin [24]. A subsequent in vivo study [25] examined the effects of implanting the material into scarred vocal folds in a canine model. The results indicated that scarred canine vocal folds were softened and showed improvement of vibratory function. The histology also showed recovery of hyaluronic acid (HA) in the lamina propria of the vocal fold. These effects were strengthened by combining the scaffold with MSCs.
Based on these findings, we implanted the material (without cells) into scarred vocal folds or sulcus vocalis in six human patients [26] (Fig. 12.9). The clinical results showed gradual improvement of acoustic parameters of voice over 6 months, although individual variation was noted. While it will be important to explore a more consistent strategy, scaffolding remains an option for treating stiffened vocal folds, and may be the most feasible method that can be applied to human subjects.
Fig. 12.9
Regenerative surgery consisting of superficial cordotomy and dissection of scar (b), implant of scaffold (c). (a) Arrow indicates sulcus. (b) Arrow indicates the vocal ligament. (c) Arrow indicates scaffold. (d) Indicates post operative status
Gelatin is a solubilized form of collagen, and may have potential as a scaffolding for the vocal fold. Zhang et al. [27] treated 12 sulcus vocalis patients with gelatin sponge implants coupled with fat injection. After 6 months of follow-up, improved maximum phonation time (MPT), shimmer, jitter, and noise ratio were reported. The effects of gelatin alone are not clear because of the combined use of fat injection; however, gelatin is known to adhere to growth factors. As will be described below, gelatin can act as a growth factor drug delivery system due to its unique characteristics.
12.3.2.2 Hyaluronic-Acid-Based Hydrogel
Hyaluronic acid (HA) has also received widespread attention as a candidate regenerative scaffold for the vocal fold. As mentioned above, HA is the key molecule for maintaining ideal viscoelasticity of the vocal fold mucosa. A group in Boston, Massachusetts has developed an HA-based “microgel” as an injectable material for the vocal fold [28]. An in vitro study with fibroblast cultures showed low or no toxicity. Mechanical measurements using a torsional wave apparatus indicated that this HA-based microgel exhibited elastic moduli similar to the lamina propria of the vocal fold at frequencies close to the range of human phonation. This study suggested that the microgel may be useful for regeneration of the vocal fold lamina propria.
A Madison, Wisconsin group has also developed HA hydrogels [29]. Chemically modified HA-gelatin hydrogels were implanted into the injured vocal folds of rabbits, and gene expression analysis of the treated vocal folds indicated upregulated levels of mRNA for procollagen type I, fibronectin, TGF-beta1, fibromodulin, HA-Synthase 2, and hyaluronidase 2. The treated vocal folds also exhibited significantly improved tissue elasticity and viscosity.
One concern of these HA-based materials is that they are artificial forms of HA and not the native version of HA that endogenously exists within the vocal fold. Unfortunately, the characteristics of native HA have not been described. It is well known that the biological behavior of HA depends on its molecular weight. Munoz-Pinto et al. [30] showed that vocal fold fibroblasts cultured in HA hydrogels showed differences in gene expression according to the molecular weight of the HA. It will be important to explore the ideal molecular weight of HA if these types of scaffolds are to be used.
12.3.2.3 Decellularized ECM (“Bioscaffold”)
Decellularized ECM is a relatively new material that has promising potential as a regenerative scaffold. Decellularization can be achieved by physical, chemical, and enzymatic processes [31]. Many recent reports have demonstrated successful decellularization of whole organs including heart, lung, kidney, liver, bowel, and skeletal muscle [32]. The technique allows production of complex 3D ECM bioscaffolds with preservation of intrinsic vascular networks as well as ECM components. Recellularization is then possible with autologous stem cells. Xu et al. [33] developed an acellular xenogeneic ECM scaffold derived from bovine vocal fold lamina propria, and confirmed biocompatibility of the scaffold with human vocal fold fibroblasts.
Badylak et al. [34] developed a porcine urinary bladder-derived ECM scaffold which contains several growth factors as well as ECM components (Fig. 12.10). We have applied this material to hemilaryngectomy defects in canine larynx, and found simultaneous regeneration of the cartilage, muscle, and the vocal fold mucosa [35] (Fig. 12.11). The primary regeneration of the mucosa was completed as quickly as 2 weeks after treatment. The vibratory property of the mucosa varied by individual, but the scaffold represents a promising material for laryngeal regeneration.
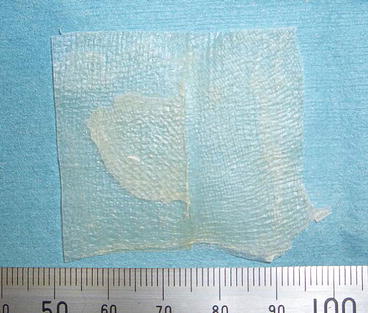
Fig. 12.10
Urinary-bladder-derived decellularized scaffold
Fig. 12.11
Reconstruction of hemilaryngectomy with decelluralized ECM scaffold. (a) Hemilaryngectomy defect of canine larynx. (b) Implant of scaffold. (c) Endoscopic findings of hemilaryngectomy. Arrow Defect after hemilaryngectomy(d) Implant (arrow) of scaffold. (e) Regeneration of the hemiglottis
The development of decellularized whole larynx has also been attempted. Baiguera et al. [36] made decellularized whole human larynx using DNAse and sodium deoxycholate, and confirmed decellularization of the cartilage, false vocal fold, and vocal fold. Preservation of the mechanical properties of the cartilage was also noted. In the future, this type of technique may enable regeneration of the whole larynx after total laryngectomy.
12.3.3 Cell Therapy
Cell therapy is the most effective tool for tissue regeneration. Cells implanted into the vocal fold mucosa can proliferate, migrate, and produce ECM proteins, which can lead to recreation of the histological architecture of the mucosa. Stem cells are expected to not only differentiate into several kinds of cells, but also to work in a paracrine manner by producing several growth factors and cytokines. Several types of cells have been studied as candidates for use in vocal fold regeneration.
12.3.3.1 Fibroblasts
We were first to report the use of vocal fold fibroblasts to restore scarred canine vocal folds [37]. The results, however, were disappointing because the vocal folds, treated by injection of autologous vocal fold fibroblasts, remained severely scarred. A group at UCLA also conducted fibroblast injections into injured canine vocal folds [38]. They used autologous buccal mucosa fibroblasts and the results were encouraging, showing improved mucosal wave of the vocal folds. The key question is how to control ECM production by the fibroblasts that are implanted into the vocal fold. Moreover, the consistent and appropriate application of mature cells remains difficult, thus many researchers focus more attention on immature cells including several types of stem cells.
12.3.3.2 Bone-Marrow-Derived Mesenchymal Stem Cells (MSCs)
It is well known that bone marrow contains mesenchymal stem cells as well as hapatopoietic stem cells. MSCs are multipotent and can differentiate into several tissues including nerve, muscle, cartilage, tendon, adipose, and cardiac muscle. It has also been shown that MSCs contribute to wound healing [39]. A population of MSCs circulates in the peripheral vessels and upon tissue damage, these MSCs migrate and home to the injury site to repair the tissue.
Another important aspect of MSCs is their reported ability to produce several kinds of growth factors and ECM such as hepatocyte growth factor (HGF), vascular endothelial growth factor (VEGF), and collagen [40]. Ohno et al. revealed that MSCs have significantly higher levels of hyaluronic acid synthase (HAS) and MMP-1 mRNA expression than vocal fold fibroblasts, which led to the hypothesis that MSC implantation would be effective for vocal fold regeneration in cases of scarring, sulcus, and atrophy [41].
Injection of MSCs into injured tissue has shown promising results. It was reported that MSCs injected around wound sites caused enhanced re-epithelialization, cellularity, and angiogenesis with increased levels of VEGF and aniopoietin-1 [42]. Another study also showed that the addition of MSCs increased collagen matrix and induced wound healing angiogenesis during early stages of wound healing [43]. Kanemaru et al. developed a cell culture system for bone-marrow-derived MSCs and treated injured canine vocal folds with an injection of autologous MSCs [44]. The results were encouraging, demonstrating better tissue recovery of the injured vocal folds. The MSCs were positive for mesenchymal stem cell markers, including CD29, CD44, CD49e, and Sca-1. Moreover, implanted MSCs in nude rat vocal folds demonstrated positive expression for keratin and desmin, markers of epithelial tissue and muscle, respectively [45]. It was further confirmed that injected MSCs are multipotent and can differentiate into several tissues including epithelium, muscle, and mesenchyme.
Hertegard et al. also treated scarred vocal folds by injection of human MSCs [46]. They found lower viscosity and elastic modulus of the treated vocal folds compared to untreated scar tissue, though the viscoelasticity did not reach normal levels. Histological analysis showed less collagen type I and in this study, the injected MSCs persisted for 4 weeks.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


