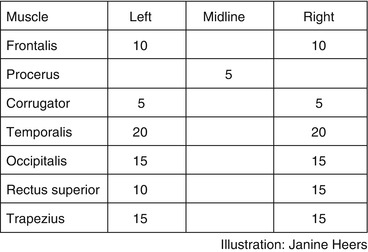
Fig. 6.1
Application of Botox (onabotulinumtoxinA) for chronic migraine according to the PREEMPT study protocol (155 IU “fixed dose, fixed site” and optional 40 IU “follow the pain”) (Illustrations by Janine Heers)
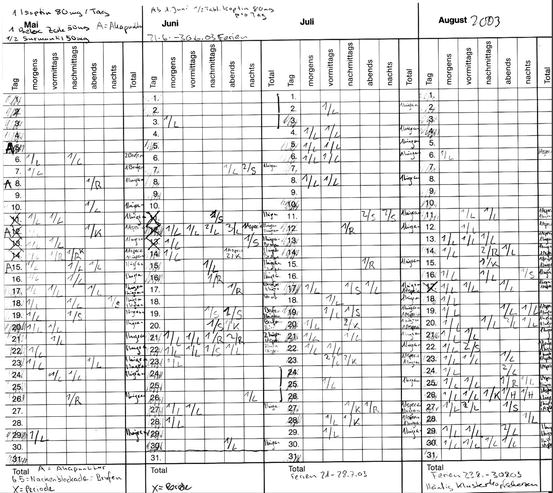
Fig. 6.2
Patient AB: headache diary before Botox treatment
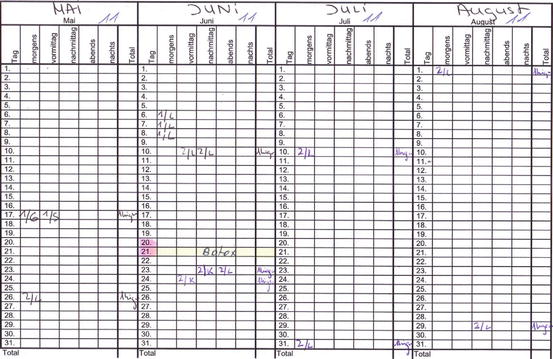
Fig. 6.3
Patient AB: Botox long-term efficacy (e.g., May to August 2011)
Case 2
Patient EG, a female born in 1960, chief dental hygienist, was started on Botox in 2004 for chronic migraine with numerous disabling attacks per month. Typically her husband had to leave his work and pick her up at her practice due to inability to continue her work or make the way home by herself. In addition to that, her husband had to pick up their daughter from day care. Injections were initiated according to a modified phase II study paradigm with 100 units. Her skin is causing extreme pain sensation to every single injection – despite pretreatment with local lidocaine ointment and ice. Nevertheless her benefits from Botox are “worth the pain” during the injections. For years she had not to be picked up at work during migraine attacks a single time. Attacks have been occurring less frequently and less disabling and are treatable with subcutaneous sumatriptan. There is a clear end of dose effect usually after 2.5 months. So far a total of 36 Botox treatments have been provided to the patient. In the year 2013, 155 IU was applied and residual tender points in the trapezius muscles additionally improved. Attack medications, mostly triptans, have been markedly reduced.
Case 3
Patient JF, a female patient born 1967, accountant, was suffering from severe chronic migraine with and without auras and severe depression for which she had in-house treatment two times. Botox was applied every 3 months since 2007, totally 25 times. Both her migraines and her depressions did improve, and since the beginning of Botox treatment, she did not require further hospitalization for severe depressions. Antidepressant medications were continued during Botox treatments until today. Under 155 IE according to the phase III Research Evaluating Migraine Prophylaxis Therapy (PREEMPT) protocol, her migraine condition further improved.
6.2 Differential Diagnosis and How to Work Up This Kind of Patient
Once diagnosis of a migraine is made (including imaging studies to rule out secondary headaches, criterion E of ICHD 1.1 or 1.2), no further diagnostic workup is needed before initiating a treatment with Botox. However, for Botox treatment of migraine, a diagnosis of “chronic migraine” (CM) is required according to the PREEMPT protocols. The most reliable tool is a patient headache diary in which the headache days can be distinguished between days with migraine and days with non-migraine headaches. Neurological exam may reveal tender points in those pericranial muscles that may receive additional dosages according to the “follow the pain” paradigm (temporalis, occipitalis, and trapezius muscles). Oral anticoagulation needs to be asked although full anticoagulation is not an absolute contraindication.
6.3 Diagnostic Workup of the Cases
Diagnoses were made according to the ICHD classification of 1988 and 2004. All patients had at least one MRI. They were all normal.
6.4 Summary of the Cases
All three cases fulfilled the criteria of chronic migraine, temporarily also of MOH. Suffering was very high and quality of life very low.
The success of Botox treatment was subjective and reported as reduction in frequency of headaches but a number of other improvements including severe episodes of depression in one case. However headache diaries provide a very useful semi-objective measure of suffering and success.
All patients try to extend the interval of Botox treatments, with success in one case but no success in the other two cases. All cases of chronic migraine changed into episodic migraine before receiving further treatments. The criterion for further treatments is usually the end of dose effect, i.e., increasing migraine frequencies while planning further treatments.
Typically patients in clinical practice will continue or start on migraine/headache prophylactic medications. There are no interactions known with any of the commonly used substances.
Botox against chronic migraine is extremely well tolerated and has numerous advantages over daily preventive medication intake.
6.5 Brief General Information
The treatment of chronic medication-resistant migraine is complicated and demanding both for the physicians and for the patients. Most CM cases bear also an overuse of attack medications (see Chap. 11 for diagnostic considerations). In this case reduction or cessation of attack medication is necessary. Treatment of CM is practically always based on medical treatment in combination with complementary approaches. Basically all preventive medications used to treat high-frequency (but still episodic) migraines are used. However, if a CM patient is seeking help from a headache specialist, many medical treatments have already been applied – without appropriate success or untolerable side effects.
Botox was introduced as a medical treatment in the 1970s for the treatment of strabismus. Botox fulfilled the two most important characteristics of an intramuscular ocular treatment: efficacy in a minimal amount and lasting effect as long as possible. Botox was consequently used to treat many different conditions characterized by muscular overactivity. In the late 1990s, William Binder in wrinkle study serendipitously discovered that by treating hyperactive facial lines in some persons, migraine improved as well. Several preliminary Botox migraine studies were made with quite conflicting results. The phase II program (only episodic migraine was included) revealed no superiority of Botox over placebo. However, it paved the ground for the phase III PREEMPT studies which showed a positive effect of 155 unit Botox over placebo. These studies lead to registration for Botox against chronic migraine by FDA (USA) and EMA in most European countries.
Botox bears several advantages over oral migraine preventive treatments: no oral intake, no known systemic interactions, perfect compliance, minimal effort (average treatment of every 3 months vs daily medication intake), and very high tolerability. Disadvantages are occasional minor and transient aesthetic changes in the face and occasional transient aches and pains in the neck. Some patients express high fears of injections or of the “poison” such that they will not try Botox. Efficacy is in the range of 50 % reduction in frequency but a number of other improvements, e.g., better efficacy of attack medications, reduced fear of the next attacks, or even psychological improvements.
Botox has been used against migraine at Hirslanden Headache Centre in Zurich since 2003 in over 1,000 patients. Originally 100 IU was applied and some patients are now switched to the PREEMPT protocol. However a number of patients with satisfying response are still treated with 100 IU. Efficacy remained high in most of the good responders. Typically patients try to extend the treatment interval beyond the typical 3 months and reschedule when they experience worsening of their migraines. Some patients for scheduling Botox treatments on demand resulting in irregular intervals. In case of very low or missing improvements, Botox treatment will be self-limiting to one or two cycles, thus limiting also the relatively high costs of this treatment option.
Botulinum toxin is so far the only medical treatment somewhat specific for the treatment of chronic migraine.
Key Points
Botox is the only approved medical treatment against chronic migraine.
Efficacy is in the range of 50 % (reduction of attack frequency by 50 %), and in approximately 10 %, practically all attacks are prevented. Long-term experience since the late 1990s and early 2000s shows persistent efficacy (over 30 treatment cycles in my personal experience).
Botox is applied approximately every 3 months. All patients try to extend the interval. In the case that Botox treatment is not effective, the treatment will be ceased after one to three treatments – and overall costs will be limited automatically.
The PREEMPT protocol (155 IU fixed dose, fixed site and optional 40 IU follow the pain) is clinically safe and useful.
Safety and tolerability are very high. Some aesthetic considerations are sometimes made by patients concerning their face and some patients may complain of neck aches temporarily.
With successful Botox treatment, savings can be made on attack treatments, urgent medical care, neurological consultations, and prophylactic treatment – in many cases weighing out substantially the previous costs caused by the patients’ migraines before initiating treatment with Botox.< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


