Refractive Surgery
Dimitri T. Azar
I. Introduction
Refractive surgical techniques have evolved rapidly over the past three decades, emerging as safer and more reliable means of treating myopia, hyperopia, and astigmatism, thus reducing the need for corrective lenses. Surgical techniques for the correction of presbyopia are under development but have not yet been refined for widespread application. Technological advances, especially in the realm of laser surgery, continue to improve precision, accuracy, and patient satisfaction. Although a wide range of refractive procedures exists, we will discuss the following refractive procedures: (a) Excimer laser photorefractive keratectomy (PRK), laser-assisted subepithelial keratomileusis (LASEK), and Epi-LASIK; (b) laser-assisted in situ keratomileusis (LASIK); (c) radial and astigmatic keratotomy (RK and AK); (d) phakic intraocular lenses (IOLs); (e) laser thermokeratoplasty (LTK); and (f) intracorneal ring segments (ICRS).
Because of the permanent nature of refractive surgery, one of its most important aspects is adequate patient selection and counseling. Many potential refractive surgery candidates have great expectations. A patient may not be a good candidate because of unrealistic expectations, or because of inadequate knowledge about the risks and benefits, or alternatives of the procedure.
Spectacles and contact lenses are reasonable alternatives to refractive surgical procedures. Not only is the accuracy of these forms of optical correction greater than that of refractive surgery, but they are also totally reversible. Although operating on a normal eye to reduce the dependence on glasses or contact lenses may seem aggressive, most patients are delighted after successful refractive surgery. To achieve uniform satisfaction with newer refractive surgical procedures, they must be validated continuously through controlled and well-designed scientific investigations to ensure better predictability and reproducibility.
The phenomenon of corneal flattening after injury with a consequent change in the refractive power of the eye was first recognized in the late 19th century. RK to correct myopia was introduced in Japan in the 1940s using anterior and posterior corneal incisions. This approach fell into disfavor 10 to 20 years later when resulting endothelial cell injury led to irreversible corneal edema and bullous keratopathy. Russian investigators improved the procedure in the 1970s by using only anterior incisions. Since its introduction to the United States in 1978, RK underwent continual refinement, but long-term studies showed significant instability and progressive hyperopic shifts that led to virtual abandonment of this surgical procedure in the late 1990s.
The excimer laser is named for the “excited dimers” of halogen gases used to generate photons of energy in the ultraviolet end of the electromagnetic spectrum. Initial excimer laser experiments with plastics revealed a high degree of ablative precision without thermal damage to surrounding areas. Early excimer laser techniques mimicking the surgical blade incisions of RK have been superseded by PRK to perform large-area central ablation for refractive correction. U.S. Food and Drug Administration (FDA) trials of PRK for myopia established its efficacy for the correction of myopia, astigmatism, and hyperopia. Subsequent FDA approvals included the LASIK and LTK techniques. Several other refractive procedures are pending approval.
TABLE 6.1 Major Contraindications to Keratorefractive Surgery | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
II. Patient selection and evaluation
Meticulous patient selection and evaluation are essential to ensure that medical and surgical requirements are met and that patient expectations match what is realistically offered by surgery.
Motivation for refractive surgery revolves around the desire to have reduced dependence on spectacles or contact lenses. This motivation may be based on occupational requirements, cosmetic or recreational needs, contact lens intolerance, or feelings of threatened safety. Patients must understand that refractive surgical procedures rarely eliminate the need for optical aids.
Contraindications. Any uncontrolled ocular surface disease, including blepharitis and dry eye, or poorly controlled glaucoma, should preclude surgery. Patients who are immunosuppressed, taking chronic steroids or antimetabolites, or suffering from connective tissue or other systemic diseases may have altered wound-healing ability that can compromise the accuracy of intended corrections. Additional contraindications include refractive instability over time and corneal ectasias such as keratoconus (KC) or contact lens–induced warpage, which may yield erratic results postoperatively (Table 6.1).
Physical examination, including manifest refraction and slitlamp biomicroscopy of the anterior segment, is performed to exclude underlying disease. To avoid overcorrection of myopia, refraction is repeated after cycloplegia.
Myopic refraction. The myopic eye brings a pencil of parallel rays of light into focus at a point anterior to the retina in the vitreous. Manifest and cycloplegic refractions aim to determine the location of the far point located between infinity and the anterior surface of the cornea. Rays that diverge from this point are brought to focus on the retina without the aid of accommodation. For the full correction of myopia, a distance corrective lens placed in front of the eye with its secondary focal point coincident with the far point corrects the refractive error. The newly created optical system allows parallel rays that come from infinity to diverge as if they originated from the far point of the eye, and thus focus on the retina. In refractive surgical procedures for myopia, the refractive power of the cornea or the crystalline lens is reduced so that parallel rays from infinity focus on the retina.
Hyperopic refraction. The hyperopic eye brings a pencil of parallel rays of light into focus at a point behind the retina. Accommodation of the eye may produce enough additional plus power to allow the light rays to focus on the retina. Cycloplegic refraction is aimed to determine the location of the far point of a hyperopic eye, which is behind the eye. A corrective lens placed in front of the eye with its secondary focal point coincident with the far point will converge parallel rays from infinity toward the far point of the eye and hence could focus on the retina without the aid of accommodation. In the prepresbyopic age group, low to moderate hyperopia is less visually significant than myopia. Older hyperopes or patients with high degrees of hyperopia that exceed their accommodative
reserve require optical correction for clear distance vision. They can benefit from refractive surgical procedures in which the corneal curvature is steepened or the power of the crystalline lens is increased to converge rays of light that emanate from distant objects onto the retina without the aid of accommodation.
Astigmatism. Astigmatism is caused by a toric cornea or, less often, by astigmatic effects of the crystalline lens. Manifest refraction will allow classification of the astigmatism as simple or compound, according to whether one or both meridians, respectively, are focused outside the retina. If one meridian focuses in front of the retina and the other meridian focuses behind it (mixed astigmatism), it is important to confirm the manifest refraction by performing cycloplegic refractions to eliminate accommodation during testing.
Binocular spectacle correction of oblique astigmatism tilts each eye’s view and may distort the perceived three-dimensional image. When astigmatism is corrected at the corneal plane, such as with contact lenses or keratorefractive surgery, full correction reduces meridional magnification and eliminates the optical distortion.
Wavefront aberration. The principles of wavefront deformation measurements, adapted from astronomical optics, will undoubtedly be incorporated in most future refractive surgical procedures. In a perfect optical system, all of the refracted rays are focused on a single plane (wavefront). Optical aberrations induce deformations on this plane and represent the optical performance of the entire visual system, not only the anterior surface of the cornea, as in most corneal topography machines. In addition to correcting second-order optical aberrations (sphere and astigmatism), higher-order aberrations (spherical aberration and coma—i.e., irregular astigmatism) can be treated (Fig. 6.1). With the use of advanced lasers and wavefront deformation measuring devices, the correction of these distortions of the human eye will continue to gain widespread use.
Cycloplegic refraction. A cycloplegic refraction is an essential part of the evaluation of a refractive surgery candidate, however, the pupil dilates and spherical aberrations are produced. The rays of light reaching the periphery of a spherical cornea and lens are bent more than the central rays. The asphericity of the cornea and lens where they flatten toward the periphery may be insufficient to counteract these spherical aberrations associated with cycloplegia. The benefit of relaxing the accommodative tone is especially important in young individuals. It may be useful to measure the cycloplegic refraction through a 3- to 4-mm aperture to account only for the accommodative tone; in this way, the effects of the peripheral cornea and the lens on the refraction are negated.
Pupil size and centration of refractive procedures. Most keratorefractive procedures are centered around the pupil under mesopic or scotopic conditions. The pupil diameter might reach 6 to 8 mm under decreased light conditions. The optical zone in a keratorefractive procedure is defined as the area of the central cornea that bears the refractive change caused by the surgery. As the pupil dilates beyond the edge of the optical zone, the rays of light are refracted differently in the midperipheral and the central cornea. This may result in edge glare and halos around objects, especially at night (or in cases of decentration of the optical zone). Some patients with particularly large pupils may have a mismatch between pupil size and optical zone diameter and should be warned about possible postoperative symptomatic optical distortions, especially under mesopic conditions.
The active reorientation of the photoreceptors toward the center of the pupil plus the possibility of edge glare if the entrance extends beyond the optic zone of the keratorefractive procedure favor the centration of refractive procedures on the pupil uninfluenced by miotics, because the center of the pupil may move in the nasal direction with miosis, which produces temporal edge glare when the pupil dilates after surgery.
Presbyopia. Presbyopia is an important aspect in relation to informed consent of keratorefractive patients. Patients over 40 years old who consider refractive surgery for myopia must appreciate the extent to which they exchange dependence on distance spectacles for dependence on near-vision spectacles. Surgically corrected
presbyopic myopes will need reading glasses as they age, whereas before surgery they could remove their spectacles to read.
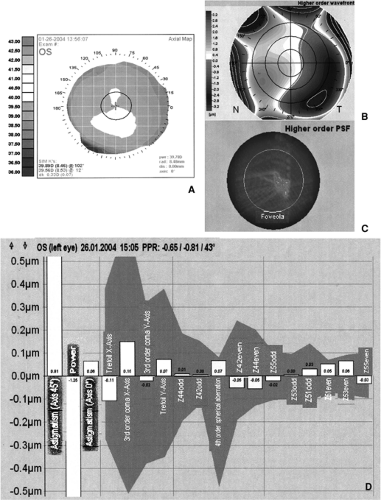
Figure 6.1. Left eye of a 42-year-old man considering customized LASIK surgery. The crystalline lens is noted to be clear on slitlamp examination. Corneal topography shows minimal surface irregularities (A). Wavefront analysis illustrates the higher-order components of his wavefront (B) and the corresponding PSF on the fovea (C). Zernike decomposition of the higher-order aberrations ≤0.15 microns RMS for third-, fourth-, and fifth-order Zernike coefficients (D). (Adapted from
Yeh SI, Azar DT. The future of wavefront sensing and customization. Ophthalmol Clin North Am. 2004 Jun;17(2):247–260).
Get Clinical Tree app for offline access


