Recurrent respiratory papillomatosis (RRP) is a rare, benign disease with no known cure. RRP is caused by infection of the upper aerodigestive tract with the human papillomavirus (HPV). Passage through the birth canal is thought to be the initial transmission event, but infection may occur in utero. HPV vaccines have helped to provide protection from cervical cancer; however, their role in the prevention of RRP is undetermined. Clinical presentation of initial symptoms of RRP may be subtle. RRP course varies, and current management focuses on surgical debulking of papillomatous lesions with or without concurrent adjuvant therapy.
- •
Recurrent respiratory papillomatosis (RRP) is a rare, benign disease with no known cure, affecting millions of children; incidence is increased with lower socioeconomic status.
- •
RRP is caused by infection of the upper aerodigestive tract with the human papillomavirus (HPV). More than 100 types of HPV have been identified; the low-risk HPV types 6 and 11 are responsible for RRP.
- •
Transmission of RRP typically occurs from mother to neonate. Passage through the birth canal is thought to be the initial transmission event, but infection may occur in utero.
- •
HPV vaccines have helped to provide protection from cervical cancer; however, their role in the prevention of RRP is undetermined.
- •
Clinical presentation of initial symptoms of RRP may be subtle, including hoarseness, dyspnea, chronic cough, or recurrent upper respiratory infections.
- •
RRP course ranges from aggressive with pulmonary involvement to isolated laryngeal disease with spontaneous remission.
- •
Current management focuses on surgical debulking of papillomatous lesions with or without concurrent adjuvant therapy.
- •
Common adjuvant therapies used currently include cidofovir and interferon (IFN).
RRP is the term used to describe infection of the upper aerodigestive tract by human papilloma virus (HPV). Although papillomas may present anywhere along the tract, the larynx is the most common location. RRP typically presents in a bimodal pattern during either adult life or early childhood. The latter presentation is marked by a more aggressive and recurring course, and therefore is commonly referred to separately as juvenile RRP. Because of this unpredictable course, knowledge and management of RRP is essential to any otolaryngology practice.
Incidence of RRP
Transmission of juvenile RRP occurs from the mother to the child either in utero or at the time of birth. The increase in prevalence of HPV cervical infections in women has been mimicked by an increase in RRP. Although it is difficult to ascertain the incidence of RRP, it is estimated that juvenile RRP is present in 4.3 per 100,000 people in the United States. As discussed later, the incidence of RRP has been greater in patients of lower socioeconomic status, another fact correlating with the increased incidence of HPV in this population. This belief was recently validated further by a pilot study of a large database of publically and privately insured patients in the United States. The study showed that the RRP incidence was higher in publically insured patients compared with privately insured patients by more than 150%: 3.21 versus 1.98 per 100,000, respectively.
The Hospital for Sick Children in Toronto showed that nearly half of juvenile patients with RRP were below the poverty line for Canadian citizens. This finding further reinforces the idea that patients of lower socioeconomic status are at increased risk. However, no correlation has been found between socioeconomic status and severity of the disease.
Economic effects of RRP
Currently, there is no cure for RRP and so treatment is directed at preventing upper airway compromise and improving vocal function while preserving laryngeal tissues. Because of the infectious and proliferative nature of RRP disease, affected patients are prone to frequent recurrences and multiple surgical treatments. This disease not only affects individual patients significantly but also places a large economic burden on their families and society in general. Typical pediatric patients require nearly 20 surgical procedures throughout their lifetimes, many of which occur early in the children’s lives. During the initial years of the disease, a child is estimated to require slightly more than 4 surgeries per year. Nearly 19% of children manifest a more aggressive course of the disease, requiring greater than 40 procedures in their lifetimes. The average lifetime cost to treat 1 patient with RRP has been estimated at $60,000 to $470,000 in the United States. On a national level, it is estimated that there are 15,000 surgical procedures performed every year in adults and children with RRP, with a total health care cost of nearly $150 million.
Economic effects of RRP
Currently, there is no cure for RRP and so treatment is directed at preventing upper airway compromise and improving vocal function while preserving laryngeal tissues. Because of the infectious and proliferative nature of RRP disease, affected patients are prone to frequent recurrences and multiple surgical treatments. This disease not only affects individual patients significantly but also places a large economic burden on their families and society in general. Typical pediatric patients require nearly 20 surgical procedures throughout their lifetimes, many of which occur early in the children’s lives. During the initial years of the disease, a child is estimated to require slightly more than 4 surgeries per year. Nearly 19% of children manifest a more aggressive course of the disease, requiring greater than 40 procedures in their lifetimes. The average lifetime cost to treat 1 patient with RRP has been estimated at $60,000 to $470,000 in the United States. On a national level, it is estimated that there are 15,000 surgical procedures performed every year in adults and children with RRP, with a total health care cost of nearly $150 million.
Research into RRP
Although certain aspects of RRP continue to remain enigmatic, the disease’s morbidity and significant economic burden are well established and underscore its clinical relevance. With any disease, some fundamental information regarding the epidemiology and virology provides a baseline for understanding. As a complex pathogen, the complete picture of the molecular mechanism of disease is still unclear; however, this aspect remains a key area of current research. Further, as a disease whose prevalence is growing, the transmission process as well as the role of recently introduced HPV vaccines is discussed. In addition, clinical manifestations and management of these patients continues to evolve with the advancement of new surgical technology and pharmaceutics.
Causes/Epidemiology of RRP
Through demonstration of papillomata on his arm, Ullman first confirmed the presence of an infectious agent in laryngeal papillomas in 1923. RRP was then confirmed to contain HPV DNA in 1980. Further characterization and typing was done by Gissman and colleagues and Mounts and colleagues, which confirmed the hypothesized role of HPV.
HPV is an icosahedral DNA capsid virus that is categorized based on genetic homology into greater than 180 identified genotypes, which correspond with different tissue preferences and clinical manifestations. HPV types 6 and 11 account for most cases of RRP. HPV-11 occurs most commonly (50%–100% of isolates) and runs the most aggressive clinical course, followed by HPV-6. HPV types 16, 18, 31, and 33 have also been reported in RRP, albeit rarely.
HPV types affecting the mucosal tracts can be broadly divided into high-risk and low-risk types based on their ability to cause malignant transformation of epithelial cells. High-risk types HPV-16 and HPV-18 are most commonly associated with cervical cancers as well as a subset of oropharyngeal carcinomas. HPV-6 and HPV-11 are considered low-risk types, not typically associated with malignancy, although transformation in RRP has been described. The rate of malignant transformation in RRP is less than 1%, and has generally been reported in adults with other risk factors such as tobacco use or exposure to radiation but also in children with prolonged, extensive disease and distal spread. The cause of transformation is thought by some investigators to follow a gradual molecular transformation. In one example, this involved integration of HPV-11 DNA into the host genome in malignant tissue samples and mutation of the p53 proto-oncogene.
In their largest series of 9 patients, Reidy and colleagues found HPV-11 to be present in all evaluable malignant samples, and RNA assays showed evidence of HPV integration in 3 of 7 sufficient samples. No evaluation of p53 status was performed in this study. In 5 sufficient samples from 7 patients with malignant transformation, Go and colleagues agreed with the consistent expression of HPV-11 in malignancy, and found p53 expression to be variable, but was not able to show a progressive histologic appearance in serial samples. The palliative treatment for benign RRP is redirected when malignant transformation occurs, using conventional head and neck cancer oncological principles that supersede the original “tissue sparing” goals. Most squamous cell carcinomas (SCCA) arising with a history of RRP are well differentiated, and, when occurring in the lung, seem to have a refractory course.
The question has also been raised regarding the presence of HPV in the clinically disease-free larynx and respiratory tree. Although ethical concerns make it difficult to explore this area in disease-free human subjects, a meta-analysis has shown that up to 10% of normal-appearing oral mucosa contained high-risk HPV. Furthermore, normal-appearing adjacent mucosa or areas appearing to be well treated may show dormant HPV when tested for HPV DNA rather than for histologic changes, as shown by the finding of HPV DNA in macroscopically normal sites in patients with RRP at a rate of 61%. This latent HPV DNA may then become reactivated and cause recurrence of papillomas. As with other viral pathogens, stress on the patient’s immune system may also serve as the trigger for the virus replication. One recent study showed that children with RRP have reduced CD 4/CD 8 ratios and poor lymphocyte response to mitogen stimulation, implying that these children have inadequate cell-mediated immunity. Thus, a deficient host immune system is likely another factor in the development of recurrent disease.
HPV Virology
The HPV is an icosahedral capsid DNA virus in the family Papovaviridae. It contains no envelope and has a double-stranded DNA genome containing approximately 8000 base pairs. HPV has a propensity for infecting epithelial cells. Although only select types are associated with RRP, more than 100 types of HPV have been identified, varying in the species they infect and the epithelial tissue they prefer. HPV infects stem cells within the basal layer of mucosa.
HPV genome
The HPV genome consists of 8 genes coding for E1, E2, E4, E5, E6, E7, L1, and L2. The L1 and L2 proteins are transcribed late in the viral life cycle and are responsible for producing the viral capsid. The E designation refers to genes that are transcribed early in the viral life cycle and are responsible for replication of the viral genome using host cellular machinery. These early genes also encode for potent oncoproteins that interact with many host cellular proteins and can cause transforming activities and disrupt cell growth and function. The most studied of these are the E6 and E7 proteins, which have been shown to prevent apoptosis and alter cell cycle function. They target the p53 and retinoblastoma tumor suppressor proteins, respectively. The tumor suppressor, p53, is an important cellular protein serving the important cellular functions of sensing and stimulating the repair of damaged DNA and triggering apoptosis of severely compromised cells.
The retinoblastoma tumor suppressor (pRb) and related pocket proteins, p107 and p130, are important regulatory subunits of the E2F transcription family members, which control cellular differentiation and proliferation. The ability of E6 and E7 to disrupt the functions of p53 and pRb, respectively, is thus necessary for promoting proliferation and uncoupling differentiation. These cellular interactions, in turn, are able to keep the differentiating keratinocytes in a DNA replicative state, which is essential for progression of the HPV life cycle. However, these same processes can lead to transformation of the cell when left unregulated, such as occurs after the physical integration of high-risk HPV viral genomes into a host chromosome.
In high-risk HPVs, the E6 protein complexes with the E3 ubiquitin ligase, E6AP, and targets the p53 protein for ubiquitin-mediated proteosomal degradation. It is the level of p53 breakdown that correlates with transformation risk. Both high-risk and low-risk E6 are able to bind p53, although only high-risk E6 proteins promote its degradation. This functional difference between high-risk and low-risk E6 is explained by the binding of these proteins to different regions within p53. Both high-risk and low-risk E6 proteins interact with the C-terminal domain of p53, but only high-risk E6 contacts the p53 core domain, an interaction that likely mediates the degradation of p53. The high-risk E7 protein binds the retinoblastoma family of proteins (pRb, p107, and p130) and also induces their proteolytic degradation, which in turn allows for cell immortalization and helps to overcome DNA damage arrest signals. Thus, cells expressing E7 are able to enter S phase in the absence of growth factors and despite the presence of inhibitory signals. High-risk E7 proteins have a greater transformation potential than low-risk E7 proteins, which correlates with the higher binding affinity of the high-risk E7 proteins for pRb.
HPV histology
Histologically, HPV appears as a pedunculated mass with fingerlike projections or multiple fronds with a central fibrovascular core covered by stratified squamous epithelium. The laryngeal mucosa appears velvety when papillomas remain microscopic, which is in contrast with the typical pinkish-whitish cauliflower presentation seen in the exophytic form. HPV also leads to a delay in epithelial maturation resulting in basal layer thickening and increased presence of nucleated cells in the suprabasal layer of the stratified epithelium.
Molecular Mechanisms of RRP Disease
Although there are limited studies dealing with the molecular pathophysiology of the HPV types involved in RRP, there is a wealth of epidemiologic and molecular data on high-risk HPV types implicated as causing cervical cancers and a subset of head and neck cancers. Cervical carcinomas harbor integrated high-risk HPV genomes within each tumor cell and continue to express the E6 and E7 viral oncogenes. As previously discussed, the high-risk E6 and E7 proteins modify the expression patterns and activities of many cellular genes and proteins to promote cell proliferation. It has been shown that both the E6 and E7 high-risk proteins are necessary for efficient immortalization of human keratinocytes.
At the molecular level, much is known about the E6 and E7 oncoproteins of the high-risk HPVs, as discussed previously. In addition to binding the retinoblastoma family of proteins (pRb, p107, and p130) and targeting them for degradation, high-risk E7 is able to bind histone deacetylase (HDAC). Together, these activities allow cell immortalization and help to overcome DNA damage arrest signals. High-risk HPV E7-expressing cells have also been shown to stabilize and increase the half-life of p53, either by disrupting the p53-specific ubiquitin ligase mdm2 or by E2F-mediated transcriptional induction of p14ARF. Furthermore, high-risk E7 is able to abrogate the cytostatic activities of certain cytokines important for restricting cellular growth and mounting an immune response to viral infection, such as transforming growth factor β (TGF-β), tumor necrosis factor α (TNF-α), IFN-α and IFN-γ, and insulinlike growth factors (IGFs). TGF-β, which is important for restricting epithelial cell growth, is resisted by high-risk E7 expression and occurs in parallel with the acquisition of resistance to differentiation cues in E7-expressing keratinocytes. TNF-β, an important mediator of immune response produced by cytotoxic T cells, also induces G1 growth arrest and cellular differentiation in normal keratinocytes. HPV E7-expressing keratinocytes continue to proliferate in the presence of TNF-β. IFNs are produced in response to viral infections. HPV E7 can subvert the cellular response to IFNs by disrupting either IFN-α–mediated cellular signaling or by downregulating the expression of IFN-β. In addition, E7 can interact with insulinlike growth factor–binding protein-3, and thus control the cellular availability of IGFs.
In addition to targeting p53 for degradation, high-risk E6 possesses redundant mechanisms for inactivating p53 and apoptosis. High-risk E6 can bind to p300, which blocks p53 acetylation and inhibits its ability to transactivate gene expression. Also, E6 proteins target the proapoptotic effector, Bak, for proteolytic degradation, thus inhibiting the intrinsic apoptosis pathway. High-risk E6 is also capable of inhibiting the extrinsic apoptosis pathway stimulated by both the Fas and the TNF-related apoptosis-inducing ligand (TRAIL) pathways. This inhibition is mediated by E6 binding to, and degradation of, both the Fas-associated protein with death domain (FADD) adapter protein and the effector caspase, caspase-8. Furthermore, it has been observed that cells expressing the high-risk E6 proteins display a reduced ability to repair DNA damage. Because the repair of DNA damage depends, at least in part, on the p53 status of cell, this may be caused by these E6-expressing cells being functionally p53 null. Despite the inability to degrade p53, the E6 protein from a range of cutaneous HPV types effectively inhibits apoptosis in response to genotoxic ultraviolet (UV) damage. This may partially be explained by the ability of E6 proteins to attenuate the UV-induced transactivation of p53-regulated proapoptotic genes Fas , PUMA , Apaf-1 , and PIG3 . Further evidence of the ability of high-risk E6 to abrogate p53 function is by activating the transcription of ΔNP73, an isoform of the p53-related protein p73, which in turn inhibits the capacity of p53 to induce the transcription of genes involved in growth suppression and apoptosis. In addition, high-risk E6 is able to induce telomerase activity in keratinocytes, which does not rely on p53 interaction but does require E6AP and is important for extending the life span of infected cells and their subsequent immortalization.
By comparison, low-risk E6 and E7 proteins are usually included in molecular studies of high-risk HPV types because of their general lack of such abilities. For example, the E6 and E7 proteins of low-risk HPVs do not seem to express cell-transforming activities that are comparable with those of their high-risk counterparts. It is also well known that the ability to promote the degradation of p53 is restricted to high-risk HPV types. In addition, low-risk E7 binds to pRb family members with lower affinity than high-risk E7 and does not target pRb for degradation. Despite these differences in function, the low-risk E6 and E7 proteins share significant homology with the high-risk proteins and retain many of the same abilities that provide redundant mechanisms for promoting cellular proliferation, disrupting apoptosis, and uncoupling cellular differentiation.
Conserved E6 functions
Both HPV-16 and HPV-11 E6 proteins bind TRIP-Br1 (transcriptional integrator of the E2F1/DP1/RB cell cycle regulatory pathway). TRIP-Br1 modulates transcription of genes relevant for G1/S transition in the same direction as the E7 protein, through disruption of E2F1 transcriptional regulation. This redundancy in function shows important similarities between high-risk and low-risk E6 proteins that are important for both the HPV life cycle and potential cellular transformation. In addition, high-risk and low-risk E6 proteins from HPV-16, HPV-18, and HPV-11 destabilize TIP60 (Tat-interacting protein 60 kDa), which relieves cellular promoters from TIP60 repression and abrogates p53-dependent activation of the apoptotic pathway. Degradation of TIP60, therefore, allows low-risk and high-risk HPVs to promote cell proliferation and cell survival. Furthermore, HPV-16 and HPV-11 E6 proteins also bind and inactivate p73, which, at the least, promotes cell growth and may contribute to cellular transformation. In addition, the ability to degrade the proapoptotic Bcl-2 family member, Bak, is conserved in high-risk and low-risk E6-expressing cells. This ability to circumvent apoptosis is important for the HPV life cycle and presumably its transformation potential.
Conserved E7 functions
HPV-6, HPV-16, and HPV-18 E7 proteins interact with PCAF (P300/calcium-binding protein–associated factor) acetyltransferase, which is a coactivator for a variety of transcription factors including p53, and thereby contributes to altered cellular gene expression and growth. Also, the E7 proteins from both high-risk and low-risk HPV types 16 and 11 interact with p300 and abolish p300-mediated E2 transactivation, which is important for differentiation-dependent activation of viral gene expression and potential cellular transformation. In addition, both high-risk and low-risk E7 proteins (16, 18, 31, and 11) bind hypoxia-inducible factor 1α (HIF-1α) and enhance HIF-1α activity via displacement of HDACs. This mechanism is important for promoting epithelial growth through activation of angiogenesis. Furthermore, introduction of either high-risk or low-risk E7 genes (18 and 6) into epithelial raft cultures induces proliferating cell nuclear antigen (PCNA) expression in suprabasal cells, which indicates the importance of the E7 protein in reactivating host DNA replication machinery in differentiated, noncycling cells. In addition, HPV-6 E7, like HPV-16 E7, interacts with and decreases the levels of p130, despite being unable to degrade other retinoblastoma tumor suppressor protein family members (pRb and p107). The ability of E7 proteins to destabilize the pRb family members depends on cellular differentiation, because both high-risk and low-risk E7 destabilize p130 in either differentiated or undifferentiated growth conditions. Only high-risk 16E7 degrades pRb in both growth conditions, whereas p107 is only destabilized by 16E7 in undifferentiated conditions. The degradation of p130 is therefore likely necessary to complete the virus life cycle, whereas the added ability of 16E7 to regulate pRb and p107 may be related to oncogenic activity.
Immune responses
Another area of molecular interest is the complex innate and adaptive immune responses made by the host with respect to HPV-6 and HPV-11 infection. It remains unclear why only a small fraction of HPV-exposed individuals develop RRP, and why still fewer develop a severe course of the disease. One explanation proposes that patients with RRP are unable to produce an effective HPV-specific T-cell response, as shown by an altered CD8 + subset and the T H 1/T H 2 cytokine imbalance found in these patients. Supportive evidence for this theory later came from comparing relative gene expression levels between papilloma and adjacent normal tissue with respect to immune responsive genes using microarray analysis. Additional studies revealed that HPV-11 E6 skews IL-10 and IFN-γ expression by patients with RRP toward increased IL-10 expression (T H 2) and away from IFN-γ (T H 1), which may be explained by an E6-induced dendritic cell dysfunction in these patients that shifts their HPV-specific immune responses toward IL-10 expression. Further evidence of a dysfunctional immune response by patients with RRP is the finding that the transporter associated with antigen presentation (TAP-1) is downregulated along with the major histocompatibility complex (MHC) class I antigen in benign papillomas. TAP-1 protein expression correlated inversely with the frequency of disease recurrence. These findings suggest that HPV may evade immune recognition by decreasing the MHC cell surface expression via downregulation of TAP-1.
Transmission of HPV
HPV is considered to be the most common sexually transmitted infection in the United States. HPV prevalence has been gradually increasing in the female population. It is estimated that the overall prevalence of HPV in women aged 14 to 59 years is 26.8%. When analyzing smaller age groups, there is a prevalence of nearly 45% in women between the ages of 20 and 24 years. These numbers also increase when factors such as education, poverty index, and marital status are taken into consideration. The prevalence increases in lower socioeconomic individuals, especially when they are unmarried and have not completed high school. In addition, one study showed that the prevalence of HPV-6 or HPV-11 in sexually active women from 18 to 25 years of age was 2.2%, whereas the prevalence of HPV-16 or HPV-18 in the same cohort was 7.8%.
Mother-to-child HPV transmission
Being a sexually transmitted disease, it has been hypothesized that HPV is transmitted vertically from the mother to the neonate during passage through the birth canal. However, this method has not been shown conclusively as the only mechanism for HPV infection. It has been shown that children born to mothers with active condylomata have an increased risk of infection, as much as 231 times that of disease-free mothers. Additional risk of infection occurs when affected primigravid mothers have prolonged vaginal deliveries, especially with an increased duration after rupture of the membrane. Such an occurrence is thought to cause further risk because the neonate spends a greater amount of time exposed to the virus. The same study showed that the risk increased to nearly double if labor lasted for greater than 10 hours. It has also been suggested that newly acquired HPV infections tend to have greater infectivity compared with chronic infections. These 2 factors alone show why low socioeconomic status (a group that has an increased prevalence of HPV) and age of the mother (increased likelihood of new-onset HPV and prolonged labor) are key risk factors for a neonate to develop RRP.
Although this knowledge helps to show the correlation between children with RRP and mothers with HPV, it implies a higher prevalence of this disease in children. However, despite how common HPV infections and active condylomata are in childbearing women, RRP is an uncommon disease entity. Further, the odds of a child contracting HPV from a mother with active condylomata have been estimated at around 1 in 400, which again suggests additional risk factors. Therefore, other factors seem likely to be important in the development of RRP: patient immunity; timing, length, and volume of virus exposure; and local traumas (intubation, extra-esophageal reflux). In addition, neonates may become infected before birth, as evidenced by a recent study showing that approximately 12% of neonates may develop HPV infections through transplacental transmission.
Caesarean section for HPV transmittal prevention
The hypothesis that HPV is transmitted to the neonate during transit through the birth canal has raised the question of whether caesarean section (C-section) may provide some degree of protection against transmission of HPV. A recent systematic review of literature was undertaken to answer this question. The investigators showed that there was no statistically significant difference between the rates of HPV transmission from HPV-positive mothers either through vaginal delivery or C-section. Of the 6 selected studies, 3 showed no difference, whereas 3 studies did show a decrease in HPV transmission with C-section. Tseng and colleagues only included women with an intact amniotic sac before undergoing surgery in the C-section group. All women with rupture of membranes before C-section were excluded because these neonates may have been exposed to the virus in the window period between rupture of the amniotic sac and time of C-section. With these criteria for the C-section group, their results still showed a significant increase in HPV transmission with vaginal delivery compared with C-section, with a number needed to treat of only 5. The findings in this study correlate with other data showing that membrane rupture even 2 hours before delivery (vaginal or C-section) increases the risk of HPV transmission.
Because prolonged exposure to HPV following rupture of the membrane can be bypassed through a C-section, it is possible that the difference between transmission rates among each type of delivery may increase when this aspect is considered. Although a planned C-section is a routine procedure, it still carries inherent surgical risks and results in increased morbidity and mortality for the mother. Further studies are needed to determine the benefit of a planned C-section in an HPV-positive pregnant woman; however, it is a topic worthy of discussion between an at-risk mother and her birth care provider.
HPV vaccine
The recent advent of the HPV vaccine is encouraging, in that it will undoubtedly affect the spread of this disease. There are currently 2 vaccines present on the market. Cervarix, a European-approved product of Glaxo-Smith-Kline, is a bivalent vaccine designed against the L1 capsid proteins of HPV-16 and HPV-18, the 2 most common causes of cervical cancer. However, although vaccination against HPV-16 and HPV-18 may help prevent cervical cancer, this vaccine does not address HPV-6 and HPV-11, the most common causes of RRP. Gardasil is a prophylactic quadrivalent vaccine with activity against HPV-6, HPV-11, HPV-16, and HPV-18. It includes recombinant virus–like particles designed from the L1 capsid protein of the 4 different HPV types. A product of Merck, it was implemented on June 8, 2006, by the US Food and Drug Administration following the findings in the phase III study and several phase II studies that prompted the Advisory Committee on Immunization Practices (ACIP) to recommend its use. Further, it was recommended that all girls 11 to 12 years old, and even as young as 9 years old, be given the vaccine along with women aged 13 to 26 years.
Although there has been a growing negative response from parents toward vaccination because of the social stigma of the disease, HPV vaccination provides an overwhelming benefit for high-risk individuals. More importantly, preventative vaccination must be administered before sexual debut regardless of age, which further raises parental concerns. About 13% of American girls are sexually experienced by 15 years, and this number increases to 43% by age 17 years and 70% by age 19 years. Also, the increase of teenage pregnancy compounds the problem of potential neonatal transmission of HPV. So although the concept of preventative vaccination of HPV seems straightforward from a medical perspective, the underlying social issues are problematic.
In addition, the vaccine has also been approved for treatment in men. The idea of vaccinating boys has been embraced by other countries, such as Australia, where it is available to boys from the age of 9 to 15 years. HPV infection among men seems to be as common as in women but is often asymptomatic, which contributes to the high rate of transmission between sexual partners. Because of its silent presentation, HPV transmission during heterosexual contact can occur without either partner being aware. The proponents of administering the vaccine to boys hope that the vaccination of both girls and boys will help slow the spread of the major serotypes of HPV.
Although each individual benefits from vaccination, it is uncertain what effect this will have on neonatal transmission of HPV or on the overall incidence of RRP. For an individual neonate, there may be an added benefit from vaccination in conjunction with performing C-section before rupture of the amniotic sac. It has been suggested that vaccines might eventually be useful in neonates for 2 reasons: (1) via transmission of immunity through maternal antibodies, and (2) through direct vaccination of neonates similar to hepatitis B neonatal vaccination. Currently, HPV vaccines are not approved for routine use on neonates, so this application requires further research.
The concept of herd immunity through vaccination of at-risk individuals should also be considered. The basis of this belief is that all women, and likely all men, from a specific age group within the population will be vaccinated. The number of those vaccinated eventually overwhelms those who are infected. As subsequent generations continue to be vaccinated, those vaccinated individuals will theoretically provide the community with immunity against the disease. Ideally, once such a community status exists, there will also be a consequent decrease in incidence of disease, in this case RRP. With these theories in mind, the HPV vaccine promises to decrease the future incidence of RRP; however, this needs further testing.
Clinical Manifestations of RRP
General respiratory symptoms in RRP
Despite becoming infected either before or during birth, most pediatric patients do not manifest any symptoms of RRP immediately. The larynx is the most common site of infection in children and, therefore, presenting symptoms tend to reflect this fact. As expected with laryngeal involvement, hoarseness is the first symptom noted; however, because of the subtle nature of this finding in a child, much less an infant, clinical suspicion for a disease process rarely arises. Other symptoms, secondary to upper airway involvement, may include dyspnea, chronic cough, recurrent upper respiratory infections, pneumonia, acute respiratory distress, dysphagia, and/or failure to thrive. Stridor, initially inspiratory and then biphasic, can be the presenting symptom of RRP and warrants significant clinical suspicion for disease and the appropriate work-up, including examination of the larynx and upper airway.
Delay in diagnosing RRP
Without a reason to suspect RRP, many patients are initially assumed to have a more common respiratory problem, such as croup, asthma, or bronchitis. Depending on the age of the child and based on the symptoms discussed earlier, allergies, acid reflux, and/or vocal fold nodules are often included in the differential diagnosis and worked up appropriately. Because of a low index of suspicion and subtle presenting signs, the definitive diagnosis of RRP is often made around 1 year after initial symptoms began. RRP is most commonly diagnosed between 2 and 4 years of age, with dysphonia being the most common presenting complaint. Most juvenile patients with RRP (75%) are diagnosed by age 5 years.
Variable course of RRP
As a highly unpredictable disease, RRP can vary in course with each affected patient. In a percentage of patients, the disease is aggressive and requires frequent debridement to protect from airway compromise. In contrast, select patients may show a progressive and sometimes spontaneous remission. Although these 2 extremes are noted, most tend to exhibit a course that lies somewhere in the middle. The course of RRP in certain patients may be further affected by the introduction of a tracheotomy or endotracheal tube. Despite the benefits of providing a secure airway, irritation and disruption of normal mucosa by these tubes increases the risk of spreading papillomas into the subglottis and proximal trachea. Nearly 30% of affected children manifest extralaryngeal spread of RRP. The most common site is the oral cavity followed by trachea, bronchi, and then esophagus. In some rare cases, the larynx may be completely unaffected, despite the presence of tracheal disease.
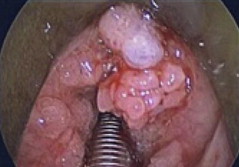
Pulmonary spread of RRP can be identified on computed tomography (CT) as noncalcified peripheral nodules that show central cavitation and air-fluid levels. Patients with pulmonary RRP incur perhaps the most aggressive course of the disease. Beginning initially with recurrent pneumonias and bronchiectasis, these patients eventually progress to frank pulmonary failure caused by destruction of underlying lung parenchyma as the disease progresses. In severe cases, malignant transformation of RRP into SCCA occurs. This typically fatal presentation is rare, accounting for less than 1% of disease presentations and is usually associated with HPV-11 infection. Figs. 1–4 show varying presentations of RRP.
P earls & P itfalls : Because of the risk of malignant conversion, it is necessary to take adequate biopsies periodically during subsequent procedures and monitor for any concerning pulmonary changes .