This review focuses on the anatomy and techniques for endoscopic resection of juvenile nasopharyngeal angiofibroma (JNA), as well as adjunctive and potential alternative treatments. JNA is a benign but locally aggressive vascular tumor that primarily affects adolescent boys. Traditionally, these tumors have been removed via open surgical approaches. Recent advances in endoscopic equipment and techniques have enabled the endoscopic surgical excision of these tumors with favorable outcomes and decreased morbidity. At our institution as at others, we have achieved successful outcomes with transnasal endoscopic resection of JNA, including tumors with significant extension into adjacent compartments.
- •
Juvenile nasopharyngeal angiofibroma (JNA) is a benign but locally aggressive vascular tumor that primarily affects adolescent boys. Preoperative embolization reduces intraoperative blood loss and should be done within 24 to 48 hours preoperatively.
- •
Preoperative angiography at the time of embolization can help to identify internal carotid artery and/or contralateral blood supply.
- •
The exact etiology of JNA remains unknown.
- •
Most JNAs can be resected via an endoscopic endonasal approach with decreased morbidity and comparable rates of blood loss and recurrence.
| GW | Greater wing |
| ICA | Internal carotid artery |
| ITF | Infratemporal fossa |
| JNA | Juvenile nasopharyngeal angiofibroma |
| NP | Nasopharynx |
| PMF | Pterygomaxillary fossa |
| PPF | Pterygopalatine fossa |
| SPA | Sphenopalatine artery |
| SPF | Sphenopalatine foramen |
Introduction
Juvenile nasopharyngeal angiofibroma (JNA) is a benign vascular neoplasm, the etiologic origin of which remains elusive. Although typically slow growing, these nonencapsulated tumors are locally aggressive, with the potential for intracranial or intraorbital extension. JNAs typically arise from the posterolateral wall of the nasopharynx and grow by extrusion via natural ostia. Advanced tumors often assume a dumbbell-shaped configuration, with one portion of the tumor occupying the nasopharynx and the other portion reaching into the pterygopalatine fossa (PPF). Intracranial extension occurs in approximately 10% to 20% of patients. JNAs typically derive their blood supply from the ipsilateral internal maxillary artery, a branch off the external carotid artery (ECA); however, bilateral supply and communication with the internal carotid are relatively common. Wu and colleagues described bilateral vascularity in 36% of patients, with ipsilateral internal carotid artery (ICA) contribution present in 10% of cases. Up to one-third of tumors have contributions from the ascending pharyngeal artery as well. As JNAs expand, they may also recruit additional blood supply from the ophthalmic and contralateral internal maxillary arteries.
JNAs are rare, representing a mere 0.5% of head and neck tumors (approximate incidence = 1:150,000) and occur almost exclusively in adolescent male patients. Isolated cases exist of JNAs presenting in female patients and older men. The most common presenting symptoms are epistaxis and progressive nasal obstruction; most patients present concurrently with both symptoms. Other presenting symptoms include nasal discharge, pain, sinusitis, otologic symptoms, visual loss, facial deformity, facial hypesthesia, diplopia (from cranial nerve compression or from direct orbital compression), and proptosis. At the time of presentation, a red-to-purple nasal mass may be visible on gross inspection of the nasal cavity ( Fig. 1 ).

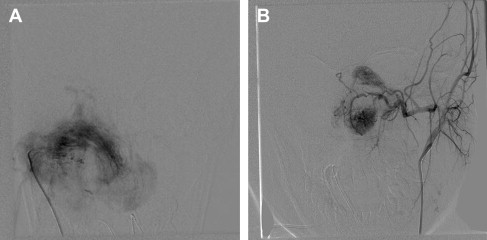
Workup for suspected JNA begins with in-office endoscopy, followed by radiographic imaging typically including both computed tomography (CT) and magnetic resonance imaging (MRI) modalities. CT scans are preferred for assessment of the extent of bony invasion ( Fig. 2 ), whereas MRI provides superior visualization of the soft tissue of the tumor itself as well as of adjacent structures such as the ICA, cavernous sinus, and pituitary gland ( Fig. 3 ). The Holman-Miller sign, anterior bowing of the posterior maxillary wall, is usually best appreciated on axial CT scan and is considered pathognomonic for JNA. Angiography provides further confirmation of the diagnosis to allow for concurrent preoperative embolization ( Fig. 4 ). Biopsy confirmation of the histologic diagnosis is not performed until in the operating room, after embolization, because of the extensive vascularity of these lesions and the potential for significant bleeding.


Surgical resection is the definitive treatment modality for JNA and is largely curative, although recurrence may occur in a minority of patients. Preoperative embolization is typically performed 24 to 48 hours before scheduled surgery to decrease intraoperative bleeding risk. In the past, resections of JNA have typically been done via open approaches. However, endoscopic approaches are quickly becoming the treatment of choice. An incision-free approach obviates the risk of growth center disruption and facial asymmetry in this young population. Furthermore, evidence suggests that endoscopic techniques may decrease operative time, blood loss, and need for transfusion, although definitive data are lacking. This review focuses on endoscopic techniques and outcomes for JNA. We also discuss potential future adjuncts to surgical treatment through genomic and hormonal translational research.
Pearls & Pitfalls : In cases in which a JNA or other vascular sinonasal tumor is suspected, one should avoid biopsy in the clinic. This is generally best done in the operating room, usually as a part of the surgical resection, because of the risk of significant bleeding.
Preoperative considerations
Staging
Several staging systems have been proposed and modified to classify JNA, and most are based on the extent and location of the tumor. The 3 main staging systems are outlined in Table 1 . The Radkowski system is the most widely used for JNA classification, dividing tumors into 3 distinct groups (see Table 1 ). The primary limitation of these older staging systems is that they were not designed for endoscopic approaches.
| Stage 1 | Stage 2 | Stage 3 | Stage 4 | |
|---|---|---|---|---|
| Onerci, 2006 | Nose, NP, and ethmoid and sphenoid sinuses or minimal extension into PMF | Maxillary sinus, full occupation of PMF, extension to anterior cranial fossa, limited extension into ITF | Deep extension into cancellous bone at pterygoid base or body and GW sphenoid; significant lateral extension into ITF or pterygoid plate, orbital, cavernous sinus obliteration | Intracranial extension between pituitary gland and ICA, middle fossa extension, and extensive intracranial extension |
| Radkowski et al, 1996 |
|
|
| N/A |
| Andrews et al, 1989 | Limited to NP, bone destruction negligible or limited to SPF | Invading PPF or maxillary, ethmoid or sphenoid sinus with bone destruction |
|
|
| Chandler et al, 1984 | Limited to NP | Extension into nasal cavity or sphenoid sinus | Tumor into antrum, ethmoid sinus, PMF, ITF, orbit, or cheek | Intracranial extension |
| Sessions et al, 1981 |
|
| Intracranial extension | N/A |
Thus, Snyderman and colleagues at the University of Pittsburgh Medical Center (UPMC) published an endoscopic staging system for JNA. They note that tumor size and the extent of sinus disease are less important in predicting complete tumor removal with endonasal surgical techniques. The UPMC staging system for JNA accounts for 2 important prognostic factors:
- 1.
Route of cranial base extension
- 2.
Residual vascularity after embolization (often signifying the presence of internal carotid or bilateral blood supply).
Compared with other staging systems, Snyderman and colleagues assert that the UPMC system provides a better prediction of immediate morbidity (including blood loss and need for multiple operations) as well as tumor recurrence ( Table 2 ).
| Stage | UPMC Staging System |
|---|---|
| 1 | Nasal cavity, medial PPF |
| 2 | Paranasal sinuses, lateral PPF; no residual vascularity |
| 3 | Skull base erosion, orbit, infratemporal fossa; residual vascularity |
| 4 | Skull base erosion, orbit, infratemporal fossa; residual vascularity |
| 5 | Intracranial extension, residual vascularity; M, medial extension; L, lateral extension |
Endoscopic Anatomy
As one considers an anterior endonasal approach, it is crucial to bear in mind the relative anatomic position of the origin, as well as the spread of a JNA.
JNAs typically originate in the area of the sphenopalatine artery (SPA) and in the area of the PPF. Most commonly, the presenting symptoms are epistaxis, resulting from the weeping of blood from this vascular tumor supplied by the SPAs, and nasal congestion, related to the blockage of 1 or both choanae.
Pterygopalatine fossa
It is important to understand the complete anatomic relationship of the PPF to fully appreciate complexities involved in resection of a JNA as well as to maintain vascular control during the procedure.
- •
The PPF is a small pyramidal space that is limited by the posterior wall of the maxilla on its anterior surface and by the pterygoid plates along its posterior surface.
- •
The ascending process of the palatine bone defines the medial boundary, and its lateral boundary is the pterygomaxillary fissure, a soft tissue space separating the PPF from the infratemporal fossa along a sagittal plane at the level of the inferior orbital fissure.
- •
The pterygomaxillary fissure transmits the internal maxillary artery from the ECA into the PPF.
- •
The anterior portion of the PPF contains the terminal division of the internal maxillary artery, the terminal branches being the palatine arteries, SPA, and posterior nasal septal artery. It also gives off an infraorbital artery that runs with the maxillary division of the trigeminal nerve (V2), as well as a small perforating blood supply to the soft tissue components within the PPF.
- •
The more posterior compartment of the PPF contains V2, the vidian nerve, and the sphenopalatine ganglion and its terminal branches. In a recent anatomic dissection published in The Laryngoscope , all neural structures of the PPF were located posterior to the SPA and lateral to the sphenopalatine foramen. This configuration allows access to the vascular structures of the PPF when dissecting in an anterior to posterior direction from an endonasal approach without direct damage to the nerves residing in the more posterior compartment. It should be noted that the number and course of the palatine nerves, as well as the branching pattern of the SPA, are often multiple and variable, ranging from 2 to 7 branches.
Understanding the relative spread outside the PPF for surgical dissection requires a comprehensive grasp of:
- •
Anatomy of the PPF
- •
JNA’s origin therein
- •
Propensity of JNAs to spread directly through natural anatomic pathways rather than through destructive invasion
Common routes of direct extension beyond the PPF include extension into:
- •
The orbit via the infraorbital fissure
- •
Infratemporal fossa via the pterygomaxillary fissure
- •
Middle cranial fossa either by traveling through the infraorbital fissure to the foramen rotundum or by traveling through the foramen ovale from the infratemporal fossa
- •
Anterior cranial vault via direct extension through the ethmoid cavity
Tumors invading the anterior cranial vault by this last route often accumulate blood supply from the anterior and posterior ethmoid arteries and extend into the planum sphenoidale or the ethmoid roof. Occasionally, extension into the palate can be seen through the descending palatine canals. However, these very small bony channels tend to be more resistant to the direct spread of JNA than the areas aforementioned. Of note, while this tumor type usually pushes boundaries rather than directly invading them, in rare cases it can invade through the periorbita or the dura.
Infratemporal fossa
Particular anatomic considerations in the infratemporal fossa include the substantial and variable blood supply coming from multiple branches of the ICA, including the ascending pharyngeal artery and the deep temporal arterial system. In addition, within the infratemporal fossa, feeders can come from the internal carotid, as well as from the foramen lacerum. Dissection laterally into the infratemporal fossa in the coronal plane is possible via an endonasal approach but often requires an anterior medial Denker’s type maxillectomy to allow for lateral access for instrumentation.
Special considerations regarding potential for skull base reconstruction
Special considerations to make while approaching the anterior cranial fossa focus on the potential need for skull base reconstruction include:
- •
If vascularized reconstruction is to be performed, one must bear in mind that embolization and surgical dissection often disrupts sphenopalatine blood supply to the posterior nasal septum and middle and inferior turbinates on the side of the tumor. Therefore, vascularized flaps should be considered from the contralateral side for dural reconstruction.
- •
If the tumor extends posteriorly into the infratemporal fossa, it can disrupt the Eustachian tube, can cause trismus, and may pick up significant blood supply from the internal carotid system. Anatomic dissections in this area require a thorough understanding of the anatomy and demand surgical dexterity to control the carotid in the carotid canal and foramen lacerum.
Pterygoid plate removal
Traversing posteriorly from the PPF, the pterygoid plates are encountered first. If the pterygoid plates are removed medially to laterally, then the muscular insertions are encountered, including the lateral pterygoid, medial pterygoid, tensor veli palatini, and levator veli palatini muscles. If the muscular attachments are dissected free and displaced laterally, this approach gives access to more posterior structures. Thus, direct access to the cartilaginous Eustachian tube is achieved, which sits between the pterygoid area and pterygoid musculature and the foramen lacerum.
Eustachian tube dissection
If the Eustachian tube is dissected from a medial to lateral plane, then the dissection follows superiorly toward its attachment at the skull base at the bony-cartilaginous Eustachian tube junction. There is an intimate relationship with the carotid canal, and the superior and posterior portions of the cartilaginous Eustachian tube are often in continuity with the inferior portion of the foramen lacerum, through which pass the carotid artery and the cervical sympathetic chain. Tumors involving this area often pick up significant blood supply from the foramen lacerum portion of the carotid artery but may also derive blood supply from the paraclival portions of the carotid. Tumors incorporating the clival portions of the carotid often have venous outflow into the clival plexus, which can be difficult to control intraoperatively.
Poststyloid parapharyngeal space
Lateral to the infratemporal fossa, behind the pterygoids, lies the poststyloid parapharyngeal space. This space transmits the carotid sheath with the carotid artery, jugular bulb, and lower cranial nerves. It is rare for a JNA to involve this area. If JNAs were to involve this area, then a combination endoscopic and lateral approach or a staged endoscopic approach should be considered.
Preoperative anatomic scrutiny
Intimate knowledge of the anatomy of the PPF as well as the surrounding anatomic spaces should be considered essential before performing resections of tumors in this area. Preoperative CT and MRI, as well as preoperative angiography, should be scrutinized by surgeons to familiarize themselves with the vascular blood supply of the tumor. In addition, these modalities allow the surgeon to assess for potential spread outside the PPF and the need to dissect critical structures such as the orbit, infratemporal fossa, or cranial vault. Posterior extension into the Eustachian tube and into the pterygoid and masticator space should alert the surgeon to a more variable blood flow with possible blood flow derived from the ICA, as well as the potential need for a combined endoscopic and open resection or staged endoscopic resection.
Preoperative considerations
Staging
Several staging systems have been proposed and modified to classify JNA, and most are based on the extent and location of the tumor. The 3 main staging systems are outlined in Table 1 . The Radkowski system is the most widely used for JNA classification, dividing tumors into 3 distinct groups (see Table 1 ). The primary limitation of these older staging systems is that they were not designed for endoscopic approaches.
| Stage 1 | Stage 2 | Stage 3 | Stage 4 | |
|---|---|---|---|---|
| Onerci, 2006 | Nose, NP, and ethmoid and sphenoid sinuses or minimal extension into PMF | Maxillary sinus, full occupation of PMF, extension to anterior cranial fossa, limited extension into ITF | Deep extension into cancellous bone at pterygoid base or body and GW sphenoid; significant lateral extension into ITF or pterygoid plate, orbital, cavernous sinus obliteration | Intracranial extension between pituitary gland and ICA, middle fossa extension, and extensive intracranial extension |
| Radkowski et al, 1996 |
|
|
| N/A |
| Andrews et al, 1989 | Limited to NP, bone destruction negligible or limited to SPF | Invading PPF or maxillary, ethmoid or sphenoid sinus with bone destruction |
|
|
| Chandler et al, 1984 | Limited to NP | Extension into nasal cavity or sphenoid sinus | Tumor into antrum, ethmoid sinus, PMF, ITF, orbit, or cheek | Intracranial extension |
| Sessions et al, 1981 |
|
| Intracranial extension | N/A |
Thus, Snyderman and colleagues at the University of Pittsburgh Medical Center (UPMC) published an endoscopic staging system for JNA. They note that tumor size and the extent of sinus disease are less important in predicting complete tumor removal with endonasal surgical techniques. The UPMC staging system for JNA accounts for 2 important prognostic factors:
- 1.
Route of cranial base extension
- 2.
Residual vascularity after embolization (often signifying the presence of internal carotid or bilateral blood supply).
Compared with other staging systems, Snyderman and colleagues assert that the UPMC system provides a better prediction of immediate morbidity (including blood loss and need for multiple operations) as well as tumor recurrence ( Table 2 ).
| Stage | UPMC Staging System |
|---|---|
| 1 | Nasal cavity, medial PPF |
| 2 | Paranasal sinuses, lateral PPF; no residual vascularity |
| 3 | Skull base erosion, orbit, infratemporal fossa; residual vascularity |
| 4 | Skull base erosion, orbit, infratemporal fossa; residual vascularity |
| 5 | Intracranial extension, residual vascularity; M, medial extension; L, lateral extension |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


