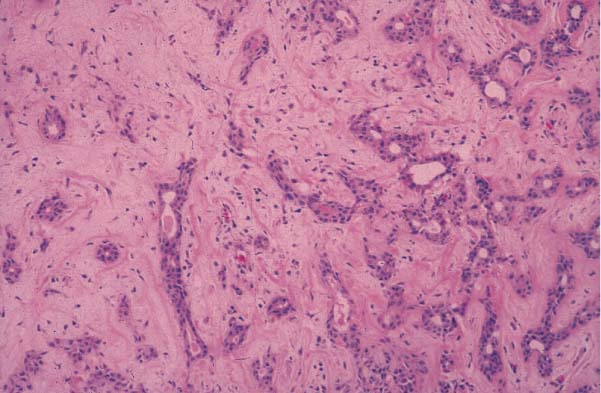
37 A 38-year-old white man consults you about nodules on the right side of his face. He indicates that these nodules have been present for several years but seem to be growing larger and are becoming a concern for him. He reports no pain, no numbness or paresthesia of the face, and no facial weakness. These nodules are located on the right side of his face anterior and inferior to his ear near a scar that he reports is from a surgery to remove a benign tumor when he was in college (Fig. 37.1). Fig. 37.1 Picture of a patient with recurrent pleomorphic adenoma. Lesions are outlined by a marking pen. His main concern with these nodules is primarily cosmetic, although when asked, he admits to being worried about cancer. He is a nonsmoker and does not have a history of much sun exposure. He cannot remember the type of benign tumor he had removed; he does remember that his lower lip was weak on the right side for several months after the surgery but eventually returned to normal. On physical examination, there is a well-healed preauricular scar consistent with a parotidectomy incision. Five palpable masses just anterior to this scar are subcutaneous and nonmobile. The largest of these masses is 1.1 cm in diameter; the remaining four are about 0.5 cm in diameter. They are nontender to palpation and located within a few millimeters of each other but clearly separate masses. Cranial nerve VII examination is normal bilaterally, and the intraoral examination is normal with no lateral pharyngeal bulge. The remainder of the head and neck examination is normal. 1. In this setting of a preauricular mass, the differential diagnosis must include all parotid benign and malignant neoplasms and cutaneous neoplasms. However, with a history of having a benign mass removed from the preauricular area, particular consideration must be given to the potential diagnosis of recurrent pleomorphic adenoma (Fig. 37.2). Fig. 37.2 Pathology demonstrating histology consistent with pleomorphic adenoma. 2. In this setting it is important to determine as definitively as possible the nature of the previously excised mass. It is important to obtain previous medical records, and if possible histologic slides should be reviewed to confirm the previous pathologic diagnosis and its benign character. 3. A fine-needle aspiration with or without ultrasound guidance is an important diagnostic step in determining the nature of these preauricular masses. This is especially important if the previous pathology cannot be confirmed. This will aid in the management planning. The important distinction is to determine whether the lesions are benign or malignant. 4. Options for imaging include ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI). Some advocate using ultrasound routinely to follow up on patients who have had a pleomorphic adenoma treated as part of the follow-up clinic visit. In this situation, when disease is clearly present or in situations when the presence of disease is suspected, MRI is the best choice for imaging. MRI has been shown to be the best imaging modality to delineate the nature and extent of parotid lesions. In cases of recurrent pleomorphic adenoma, the palpable lesions may just be the “tip of the iceberg” and MRI has been shown to best demonstrate the nature of multiple lesions. 5.
Recurrent Pleomorphic Adenoma
History

Differential Diagnosis—Key Points
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


