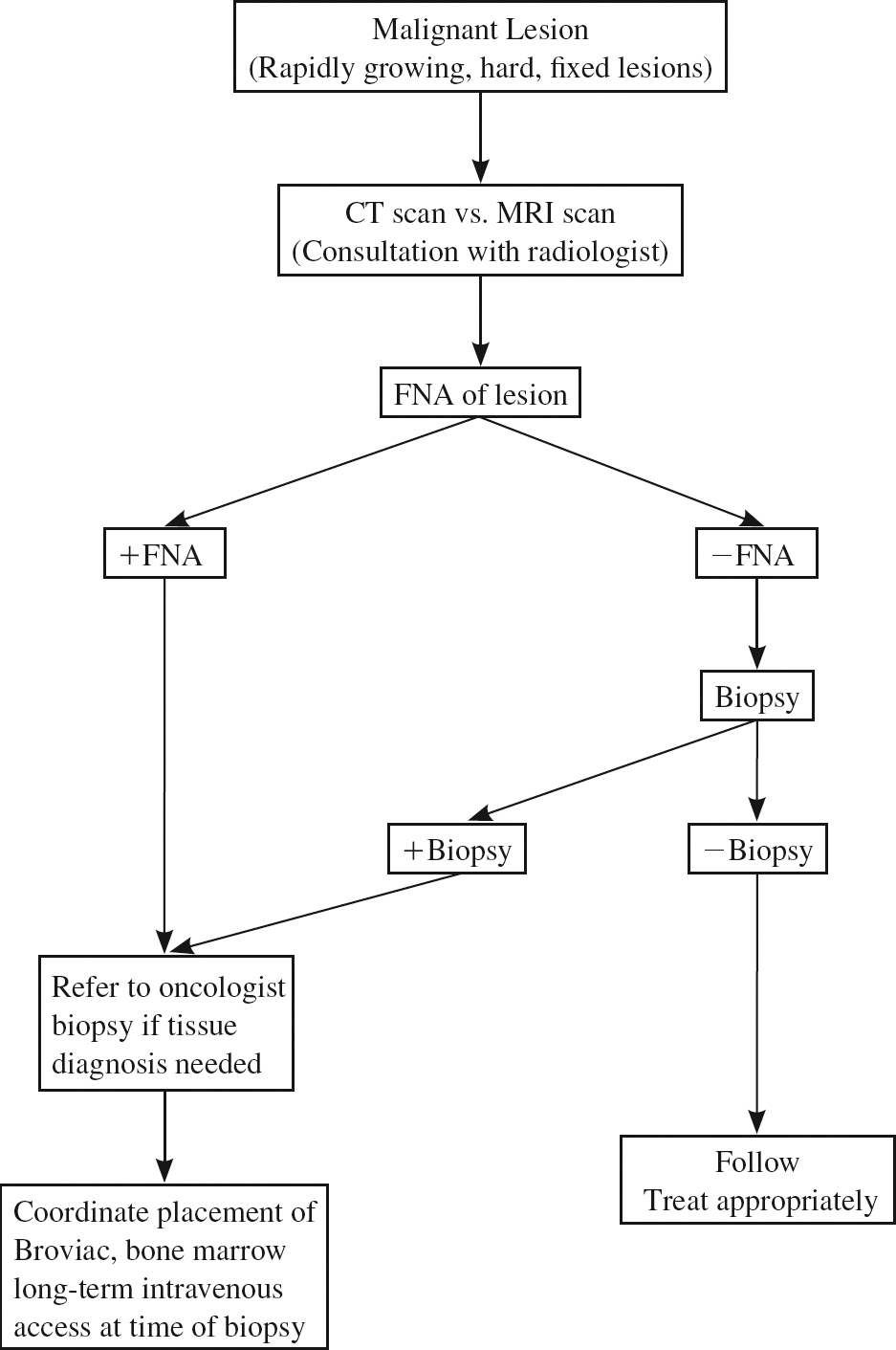
46 Recurrent Neck Masses in Children The management of recurrent neck masses in children can be difficult. One must weigh the concerns of malignancy against the possibility of overtreatment of these lesions, which will overwhelmingly be benign. This chapter uses four sample case studies to examine the main types of masses: inflammatory, congenital, and malignant. It is estimated that 50% of all 2-year-old children have palpable cervical adenopathy.1 Inflammatory masses are usually associated with signs of an upper respiratory tract infection, such as fever, rhinorrhea, and tenderness over the mass. The mass can be warm to the touch with associated overlying erythema and edema. Congenital lesions are usually slower growing and on appearance are soft. Malignant lesions show persistent growth and are commonly fixed and hard to palpation. In the surgical management of neck masses, care should be taken to preserve landmarks that may be useful if the masses reoccur. In evaluating recurrent neck masses in the postoperative period, a thorough evaluation should be obtained to rule out complications of surgery as compared with a recurrence (i.e., a seroma or stitch abscess that may mimic a recurrent mass). Palpable lymphadenopathy in the neck is a common finding. Any lymph node > 10 mm is characterized as cervical adenopathy.2 The most common cause of cervical adenopathy in children is a viral infection of the upper respiratory tract. Most viral infections run their course within 7 to 10 days, and cervical adenopathy will usually resolve with the resolution of the virus. In a smaller number of cases the lymphadenopathy will remain for weeks to months, prompting visits to the physician for consultation. The more common viruses causing lymphadenopathy are Epstein-Barr virus, enterovirus, adenovirus, and human immunodeficiency virus (HIV). Bacterial infections of the upper respiratory tract are also associated with cervical adenopathy. Bilateral cervical adenopathy is a frequent finding in children with group A β-hemolytic strep pharyngitis. Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis are the most common organisms causing otitis media and sinusitis. Unilateral or bilateral cervical adenopathy can be associated with these infections as well. Staphylococcus aureus and group A Streptococcus are implicated in 60 to 85% of cases of unilateral cervical adenitis in children.3 These infections usually occur when infection drains into a lymph node from a proximal site in the head and neck. These nodes are warm to the touch, soft, and painful. Cervical adenitis from these two organisms can be seen more commonly in neonates and young children.4 Unilateral cervical adenopathy can also be due to mycobacterium infections, cat scratch fever, and toxoplasmosis. Atypical mycobacterium infection is more commonly associated with unilateral cervical adenitis. These nodes are usually slow growing, with overlying erythema and thinning of the skin. If left untreated, fistula formation may occur. The diagnostic work-up for children with recurrent neck masses requires a thorough history and physical exam. The findings of infection in other sites of the head and neck point to the primary cause of cervical adenitis, and appropriate culture and treatment should be undertaken. For children who have failed antibiotic therapy, a thorough laboratory evaluation for other infectious etiologies should be undertaken. This should include an evaluation for Epstein-Barr virus, cytomegalovirus (CMV), toxoplasmosis, and HIV. A computed tomography (CT) scan or magnetic resonance imaging (MRI) should be performed to more completely evaluate the mass and plan medical and, if needed, surgical therapy. If possible, the original CT and/or MRI should be obtained and compared with the postoperative films in the evaluation of recurrent masses. In the immediate postoperative period (i.e., the first 3 months), an ultrasound may be helpful to rule out a postoperative seroma. A 15-month-old female was presented to her pediatrician with a 4-day history of temperature to 104°F (40°C) and left neck swelling. She was diagnosed with cervical adenitis and started on antibiotics. The swelling worsened, and the child was admitted for intravenous (IV) antibiotics. Urine, blood, and cerebrospinal fluid (CSF) cultures were all negative. Her white blood cell (WBC) count was 10.9, and a chest x-ray was negative. Her condition worsened, and she was transferred to a tertiary care hospital for further evaluation. Upon admission she was noted to have profound neck and facial swelling with respiratory distress from swelling in the floor of the mouth. She was brought to the operating room, where direct laryngoscopy revealed significant laryngeal edema. A tracheotomy was performed as well as incision and drainage of her neck abscesses. The patient was begun on clindamycin and cefuroxime. A CT scan was performed. Initial cultures grew only S. aureus, and the purified protein derivative (PPD) was negative. The patient was returned to the operating room 1 week later for extensive débridement of her neck. She was maintained on IV antibiotics and slowly improved. She was decannulated 1 month after admission and discharged to home. Decision tree for initial presentation A 2-year-old female was transferred to a tertiary care hospital with persistent fevers and neck swelling following incision and drainage of a right lateral neck mass. The patient had a 4-day history of an upper respiratory tract infecction with fever and progressive neck swelling. She was started on oral antibiotics by her pediatrician with continued progression of her fevers and neck swelling. The child was admitted to a local hospital, where she was brought to the operating room, and incision and drainage of her right neck mass was performed. Postoperatively, she continued with fevers to 104°F (40°C) and an elevated WBC count. She was transferred to a tertiary care hospital for evaluation. Upon admission her WBC was 23,000, and she was febrile to 100.4°F (38°C). The right neck revealed a healing incision but was indurated and erythematous. A CT scan revealed a deep neck abscess as well as a continued small collection at the site of the previous incision. The patient was brought to the operating room, where neck exploration and drainage of the neck abscess with placement of a Penrose drain in the site occurred. She was maintained on a 10-day course of IV antibiotics, and the drain was removed on the 3rd postoperative day. Her fevers defervesced, and she was discharged home on postoperative day 10. The most common congenital lesions of the head and neck are lymphangiomas, hemangiomas, thyroglossal duct cysts, and branchial cleft cysts. Hemangiomas are the most common tumor of infancy. They have three phases of growth: rapid proliferation (3–9 months), a quiescent period of variable length, and a spontaneous, slow involution phase (18 months–10 years). MRI is extremely useful in confirming the diagnosis of hemangiomas.2 Treatment of hemangiomas is required only if they impinge on vital structures (i.e., the subglottic space or orbit), as the vast majority will resolve without intervention. Venous malformations are located in the head and neck in 40% of cases. They are considered to belong to a group of benign vascular tumors that form in the head and neck. Physical examination reveals a soft, compressible mass that is red to bluish in color. Venous malformations do not undergo spontaneous involution as compared with hemangiomas. Diagnosis can be made by the use of MRI and CT. Treatment of these lesions requires a multimodality approach, including surgery, sclerosing agents, and medical therapy.2 Approximately 75% of lymphatic malformations occur in the neck. They are postulated to develop from sequestered lymphatic sacs that fail to communicate with peripheral drainage channels. Lymphangiomas are usually present at birth but can appear as late as 2 years of age.3
Inflammatory Neck Masses
Case 1
Case 2
Congenital Neck Masses
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine
