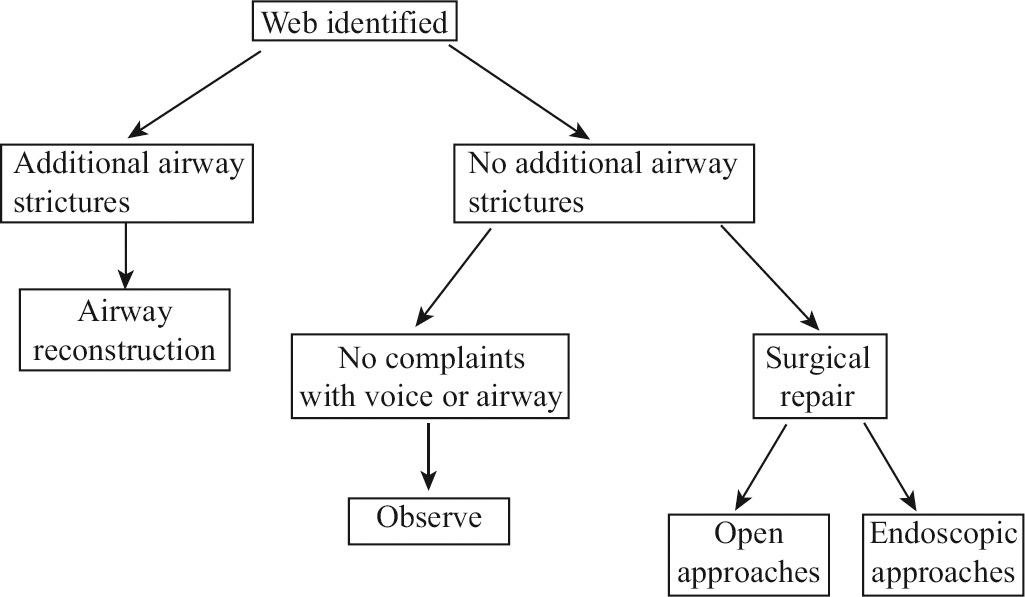
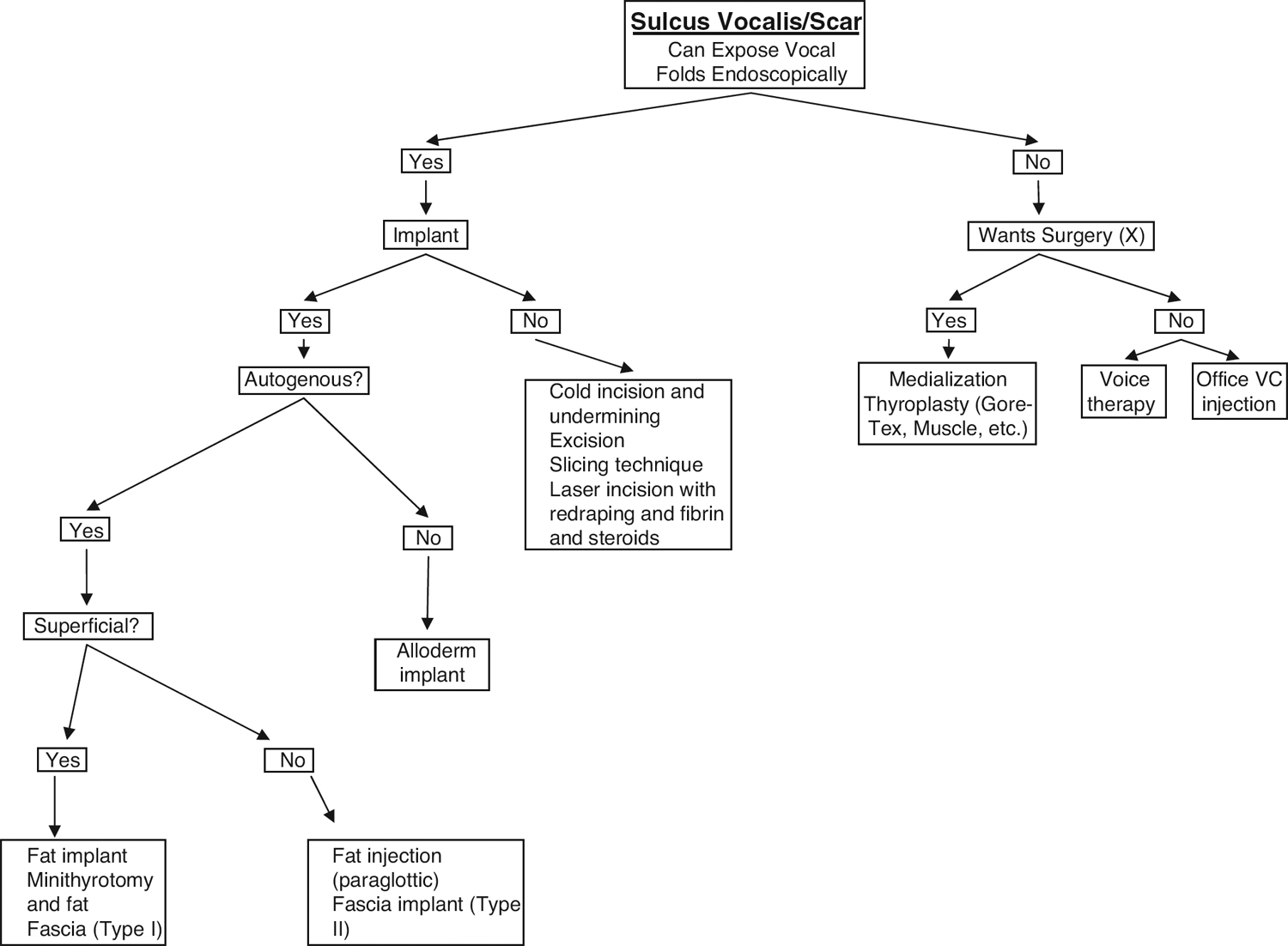
3 Recurrent Benign Glottic Lesions Recurrence is either a real or an illusory phenomenon. A lesion may actually return after treatment, or it may simply not have been identified initially. The larynx has special properties that predispose it to benign recurrent lesions. First and foremost, adequate exposure to the larynx in an office setting has always been limited by lighting and by maneuverability of the examining instrument. Although mirror exam often provides a panoramic view with excellent color resolution, patient comfort limits the time available for evaluation. Furthermore, there is no permanent and reproducible record of the examination. Flexible fiberoptic examination allows for an extended examination and less interference with normal laryngeal biomechanics. However, the pixellated image produces worse resolution, and the color can be distorted. A permanent record is possible with this technology. Rigid stroboscopic examination with a rod-lens system permits excellent lighting, a digital recording medium, and the ability to examine subtle pathology at the glottal level. The increased cost, difficulty in interpreting the images, and controversy regarding the value of stroboscopy have influenced the availability of this tool. Nevertheless, it should be regarded as the method of choice in evaluating especially elusive or confusing laryngeal pathologies. Laryngeal lesions judged to be “recurrent” simply might not have been noticed or fully evaluated on primary inspection. Second, some conditions are simply not common; as the saying goes, “The eye cannot see what the mind isn’t prepared for.” There is a background of considerable controversy and confusion regarding the etiology of such lesions as vocal process granulomata, glottal nodules and polyps, narrowing of the anterior larynx, and sulcus deformities. With this background in mind, there are widely divergent strategies for treatment. When there are divergent strategies and lesions are uncommon, it is easy to see why a consensus viewpoint is a difficult goal and why lesions may not be treated optimally and may recur. Lastly, the presence of vocal trauma from overuse and the influence of laryngopharyngeal reflux disease may create an environment predisposing to recurrence. Vocal process “contact ulcer” and vocal process granuloma (VPG) are most likely different manifestations of the same disease process. Although never definitely proven by serial biopsies and histologic examinations, a contact ulcer as described originally by Jackson in 1928, is a superficial erosion of the mucosa overlying the vocal process of the arytenoid cartilage.1 This erosion turns into an aggregation of granulation tissue in the same place: a vocal process granuloma. It may occur unilaterally or bilaterally. An inciting event, whether iatrogenic (e.g., intubation) or spontaneous (e.g., vocal hyperfunction, violent cough) may cause the initial injury to the site. Aggravating factors are considered to be many, including chronic throat clearing, a low-pitched voice, a hard glottal attack, voice misuse in general, laryngopharyngeal reflux, smoking, and the chronic infection of the exposed cartilage. Therapies have thus been designed to address these aggravating factors. They include voice rest, voice therapy, medical management of allergy and sinus disease, medical management of laryngopharyngeal reflux, and botulinum toxin injection to reduce physical trauma on the arytenoids during adduction. A biopsy has been recommended to rule out malignancy. There is evidence to suggest that the disease may be from a perichondritis of the exposed arytenoid cartilage. The clinical presentation of VPG can be a varied one. In his 40 years of clinical practice, Chevalier Jackson, who first described the entity in 1928, saw 127 cases.1 He described it as a uni- or bilateral lesion that was best seen on abduction of the vocal folds. “Diffuse symptoms,” as described by Ylitalo and Lindestad, are vocal fatigue, vocal discomfort, the need for excessive throat clearing, and the sensation of a foreign body in the throat.2 Other common symptoms included hoarseness, uni- or bilateral throat pain, hemoptysis, dyspnea, and cough. This group of patients is often considered to be high-functioning professionally and to have a component of emotional stress responsible either for the initial damaging event or for its propagation. The vocal dysfunction can endanger the livelihoods of voice users. Additionally, the pain and general discomfort of an often-prolonged disease course, with the high likelihood of recurrence, can make this benign disease debilitating. When lesions on the vocal process are noted early, they are called contact ulcers and are superficial erosions of the mucosa overlying the vocal process of the arytenoid. Even the original term contact ulcer speaks to its origin through physical trauma to the area. With time and aggravating factors, these contact ulcers may progress to VPG. Although there are no studies of serial histologic examinations of these ulcers as they progress, the clinical observation is that the originally superficial contact ulcers gradually enlarge as granulation tissue forms at the vocal process of the arytenoid cartilage and just superior to it. Ylitalo and Lindestad defined two different sites of the disease, one at the vocal process itself and the other posterosuperior to the vocal process.2 They noted 25% and 75%, respectively. The development of reactive tissue at this site is presumed to be from the inflammatory cascade. Decision tree for anterior glottic webs Decision tree for sulcus vocalis Von Leden and Moore performed cinefluoroscopic examination of larynges during phonation of patients with VPG.3 The laryngeal movements were assessed for the quality of motion of the arytenoids. These patients were noted to have a hard glottal attack and often what appeared to be significant force at the level of the arytenoids when using a low-pitched voice. Although no empiric data were derived from this study, the suggestion was made that a constant physical event was occurring at the level of the vocal process. Furthermore, the force involved might be responsible for the continued growth of the exuberant tissue at that site. It has also been noted that men have the disorder more often than women. Hirano et al observed that the larynx achieves closure just above and posterior to the level of the true vocal folds, which implies that it is the arytenoids helping to achieve this closure.4 The posterior glottic chink seen in women is a gap between the arytenoids during adduction. This gap may create a situation where the vocal processes simply do not make as much surface area contact as in men and may not be subject to the same irritating events. Additionally, women have higher pitched voices that do not require the adduction force of the arytenoids that von Leden and Moore described with low-pitched voices.3 Evidence to support the irritative etiology of this disease is also put forth by Ward et al, who described cinephotographic and cinefluoroscopic evidence that chronic throat clearing and repetitive coughing are violent and frequent events to the larynges of patients suffering from VPG.5 The lead author invokes his own experience with laryngopharyngeal reflux (LPR) disease as a possible source for coughing and throat clearing. He claims that the constant irritation causes choking, violent coughing, laryngospasm, and overactive use of the larynx. Fluoroscopic evidence of hiatal hernia with visualization of gastric contents into the larynx helped to confirm a source of inflammation. No prospective pH studies have been performed to date to compare data with his observations and techniques of evaluation. However, gastric acid as a possible cause of VPG was demonstrated by animal studies. Delahunty and Cherry performed a study of application of gastric acid to the posterior vocal fold of two dogs.6 Saliva was applied to the vocal fold of the control dog. After 29 applications, an appearance very similar to that of VPG developed, suggesting that the presence of gastric acid in the larynx may be responsible for VPG. There was no such appearance in the control dog. This is the only such study reported, and the significance of acid reflux has yet to be definitely proven either in its causality or in its perpetuation of the disease. The fact that the disease arises from chronic irritation is, however, difficult to ignore. Radiographic evaluation of the larynges of these patients suggests that the vocal processes themselves have been subjected to irritation.7 Normal arytenoids are composed of hyaline cartilage in the body and elastic cartilage at the vocal process. Elastic cartilage does not normally calcify. Computed tomography (CT) scans of five patients with VPG showed calcification of the vocal processes of the arytenoids. This finding suggests that a chronic inflammatory process to that region had transformed it into an area capable of being calcified. In the diagnostic work-up and follow-up of patients with VPG, the use of a validated tool, such as the Voice Handicap Index (VHI), might provide longitudinal information regarding their presenting symptoms and improvement. Additionally, the routine use of esophageal probes to document LPR disease in scientific studies might validate the suspected role reflux plays in this entity. As the supposition of chronic irritation is an attractive and justifiable one, however, therapies should be directed toward the possible inciting agents. Jackson himself recommended absolute voice rest as the mainstay of primary therapy for these patients, under the assumption that vocal use or misuse perpetuates the disease.1 Voice therapy has been explored as the primary therapy for VPG with mixed results. Ylitalo and Lindestad retrospectively reviewed 123 patients with VPG.2 Twenty-nine out of 120 patients not cured by surgery used only voice rest as their therapy. The remaining 91 were patients who recurred after surgery or who chose voice therapy as their only treatment. At 6 months, the cure rates for these three groups of patients were 24%, 23%, and 29%. These results changed to 31%, 35%, and 51% at 12 months and 34%, 50%, and 58% at 18 months after voice therapy. This suggests that either voice therapy may take a long time to help heal the ulcer or simply that time will cure most of these lesions. Additionally, the recovery time was twice as long for patients who had undergone surgery as for patients who had not had surgery. It should be noted that the recurrence rate after surgery was 92% and that this was a retrospective study. Peacher documented the progress of 70 patients with VPG to voice therapy and arrived at similar conclusions.8 She found that with enough time (follow-up from 1 to 12 years), 65 of 70 patients healed completely and did not recur. Also, the patients who received surgical intervention of at least one operation took 6.5 months to heal compared with 2.5 months for those who had no operations. Peacher also observed the healing rate was the same for patients who received concentrated voice therapy versus those whose appointments were more spread out. Also, the more operations a patient underwent, the longer was the healing time. No antireflux therapy was administered. Antireflux therapy has been supported as a mainstay for the treatment of VPG, but no studies have prospectively shown its efficacy. Although Delahunty and Cherry’s dog study is suggestive, the role of LPR in the propagation of VPG remains to be seen.6 Botulinum toxin A (Botox) injection has been introduced with favorable initial results. Botox has been used in the thyroarytenoid muscle and lateral cricoarytenoid muscle to control the hyperdynamic state of the larynges.9 Six patients were included in the study by Nasri et al, and all were cured of the VPG, with three patients having follow-up of less than 1 year. The treatment with Botox amounts to chemical voice therapy. Botox stops the hyperadduction of the arytenoids and decreases the force with which the vocal processes collide. It may be useful for refractory cases, as it is not without risks, which include a breathy voice, dysphagia, and reaction to the drug itself. Topical inhalant steroid therapy with budesonide has been used for the treatment of VPG.10 In a prospective study, 20 patients were given the topical inhalant 4 times a day (two puffs of 50 mcg), and a control group of 14 patients received voice rest, antacids, “anti-inflammatory agents,” and oral corticosteroids. In the treatment group, the VPG disappeared completely in 19 of 20 patients (95%) at 1 year. In the control group, 6 of 14 patients (42.8%) were free of granuloma at 1 year. Microlaryngeal surgery was performed on the eight failures in this group, resulting in six successes out of eight in this subgroup. The only side effect was oral monoliasis in two patients who received the steroid inhalant. A success rate of 95% is indeed impressive and represents the highest reported rate. Radiotherapy has been used for treatment failures with some success. Obvious disadvantages include induction of malignancy and exclusion of radiation therapy should the patient develop an upper aerodigestive tract cancer in the future. A typical radiation course would be a total of 12 Gy in four daily fractions using 6 MV photons centered on the larynx.11 Radiation has been used to treat other inflammatory conditions, such as keloid scarring, heterotrophic bone formation, and conjunctival pterygia. These conditions are similar to VPG in that they are benign inflammatory processes that result in tissue proliferation. The suggestion of the authors is to first surgically debride the area and then radiate. Clearly, this approach is not suggested for all cases, but it can be considered in treatment failures. A less invasive and repeatable intervention is now possible with office-based laser therapy. The 585 nm pulsed dye laser was designed to target vascular lesions of neonatal skin. It was initially applied to papillomatosis of the larynx under microlaryngoscopic conditions, as the fibrovascular cores of each frond are prime targets. The flexible fiber has been adapted to pass through the working channel of flexible transnasal endoscopes, allowing for application of the laser to laryngeal lesions with only topical anesthesia.12 In a preliminary experience with this laser in 10 patients with VPG, Clyne et al showed complete resolution of VPG in 5 cases and partial response in 3 cases, with no change in 2.13 Although the technology is sound, this approach should be viewed as adjunctive to voice therapy because control of vocal hyperfunction and reflux is likely to produce the most reliable long-term results. Initial inciting events may be difficult to prevent, but aggravating factors may be addressed. The pathophysiology is still unclear, and no histologic studies have been performed to prove the development of VPG from contact ulcer. It should be noted that repeated resection either with the laser or with a “cold” technique does not eradicate the disease, and surgery as a sole therapy should be avoided. No randomized controlled trial of different treatments such as antireflux therapy with and without voice therapy has been undertaken because of the uncommon nature of the disease and the need for a multi-institutional trial. It may be true that no therapy would produce the same results as those practiced to date. However, considering the years of experience and the evidence that repetitive trauma and irritation cause VPG, and that antireflux management, voice therapy, inhaled steroids, Botox, and 585 nm pulsed dye laser have shown some efficacy, clinical trials to optimize care can be of significant value. Benign lesions of the glottis include cysts, nodules, and polyps (Figs. 3.1, 3.2). (Because keratin cysts are derived from epithelial rests and do not recur once excised, nodules and polyps are more central to the discussion of recurrent lesions. Nodules and polyps are believed to appear in the hyperkinetic larynx where microtraumatic events to the vocal folds do not heal within the extracellular matrix of the lamina propria. Furthermore, the dysfunctional state that the nodules and polyps create only exacerbates the hyperkinetic habits of these patients. In an effort to compensate for the dysfunctional voice, greater effort is exerted, and the condition worsens. Many authors have noted anecdotally an association between hyperkinetic voice use and nodules and polyps.14–16 Few hard data exist, however, even from an epidemiological standpoint, to justify this association. More recent examinations of histologic sections, however, point to microtrauma of the vocal folds as the central culprit, confirming the suspicion that overactivity may be at the root of these benign growths.17
Vocal Process Granuloma
Clinical Evaluation
Etiology
Treatment
Nodules and Polyps
Etiology
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine
