(1)
St. Johns, FL, USA
(2)
Helen Keller Foundation for Research and Education, International Society of Ocular Trauma, Birmingham, AL, USA
(3)
Consultant and Vitreoretinal Surgeon, Milos Eye Hospital, Belgrade, Serbia
(4)
Consultant and Vitreoretinal Surgeon, Zagórskiego Eye Hospital, Cracow, Poland
56.1 General Considerations
In eyes with a posterior staphyloma, the rigid ILM does not allow the otherwise elastic retina to stretch and conform to the highly concave contour of the scleral bulge (see Fig. 56.1).1 The detachment typically develops over the entire area of the staphyloma, and a secondary macular hole may eventually also form.
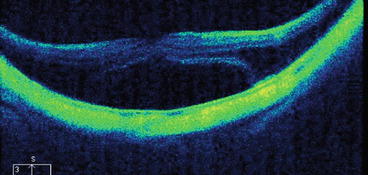
Fig. 56.1
OCT image of an eye with a central RD over a posterior staphyloma. The retina is unable to follow the large bulging of the eyewall and the neuroretina gets detached from the choroid/RPE with serous fluid present in the subretinal space. The curved line of the hyper-reflective RPE layer is due to the posterior staphyloma
Pearl
In all other forms of RD the primary cause is either in front of the retina (VR traction), below it (subretinal traction or mass), occasionally inside the retina (shortening), or fluid production (optic pit); here the cause is an anatomical abnormality in the eyewall.
One possible surgical option is to place a buckle over the macula. I prefer performing PPV for this condition; the technique is described below. The main goal is to relieve the central retina of the two forces that prevent retinal reattachment: the posterior cortical vitreous2 and the ILM.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


