The authors present the value of imaging for preoperative evaluation of structures that are not assessed or incompletely assessed on physical and endoscopic examination. Discussed are CT, MRI, and positron emission tomography–CT and the appropriate selection of each method to provide information, including the presence or absence of extent of disease to the pre-epiglottic and paraglottic spaces and the subglottis, cartilage invasion, extralaryngeal spread of disease, nodal metastasis, and tumor volume.
Clinical examination (including endoscopy and biopsy) of the larynx allows an accurate assessment of superficial spread of neoplasm. Pathologic involvement of the deep spaces of the larynx is greatly underestimated by the clinical examination, however. Imaging, conversely, fails to detect superficial mucosal disease and tends to overestimate the deep extent of tumor. The combination of information from cross-sectional imaging when taken together with information gleaned from clinical examination provides the most accurate pretherapeutic staging of laryngeal neoplasm. For this reason, close collaboration with a radiologist skilled in the performance and interpretation of imaging of the head and neck is especially vital to direct successful therapy of patients who have neoplasm of the larynx.
Imaging anatomy of the larynx
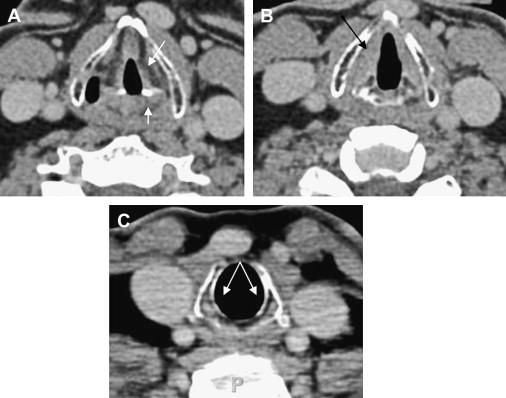
The larynx is a hollow tube lined by mucosa and adapted for protection of the airway and phonation. The cartilaginous scaffolding of the larynx is composed of the thyroid, cricoid, and arytenoid cartilages surrounded by connective and muscular tissue that form its walls. Superiorly, the epiglottis demarcates the boundary with the pharynx. Inferiorly, the larynx extends to the lower margin of the cricoid. Laryngeal anatomy is divided into supraglottic, glottic, and subglottic regions ( Fig. 1 ).
Supraglottis
The supraglottic larynx extends from the epiglottis and laryngeal surface of the aryepiglottic folds superiorly through the laryngeal ventricle inferiorly. The supraglottic larynx is delimited inferiorly by the superior surface of the true vocal cords. On cross-sectional imaging, the false vocal folds are easily discriminated from the true cords by submucosal presence of fat in the former. The pre-epiglottic space is filled with fat tissue ( Fig. 2 C). Robust lymphatic drainage to the high deep cervical chain contributes to the higher incidence of nodal metastasis at the time of diagnosis of lesions in this region.
Glottis
The vocal folds (true vocal cords) and anterior and posterior commissures comprise the glottis ( Fig. 2 A, B). Superiorly, the glottis is bounded by the supraglottic larynx; inferiorly, it is bounded by the subglottic larynx. Radiologically, the vocal folds are easily distinguished from the false vocal cords by the presence of submucosal soft tissue density attributable to the vocalis muscle. Lymphatic drainage from the glottis itself is sparse, and nodal metastasis from lesions in this region is rare.
Subglottis
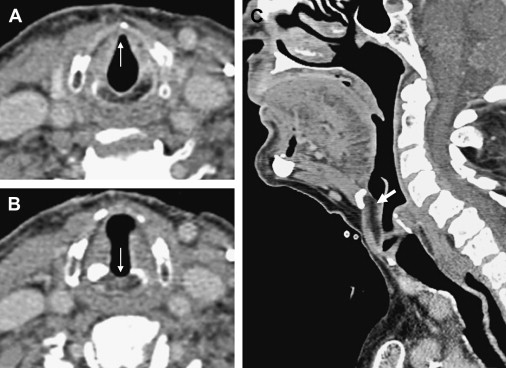
The subglottis extends from the inferior surface of the vocal fold to the inferior extent of the cricoid cartilage and is difficult to visualize in the office. The endoluminal contour of the subglottis is normally smooth (see Fig. 1 C). The presence of subglottic soft tissue should raise suspicion of neoplastic invasion. Lymphatic drainage from the subglottis is sparse, and nodal metastasis from lesions in this region is rare.
Choosing modality of imaging
CT versus MRI
State-of-the-art multichannel CT affords high spatial resolution images that can be reformatted in any desired plane, essentially negating the traditional advantage of MRI because of its multiplanar capability. Superior contrast resolution and multiparametric imaging (eg, T1-weighted, T2-weighted) remain significant advantages of MRI.
CT evaluation is much faster than MRI, substantially reducing or eliminating artifacts of movement attributable to breathing, swallowing, or coughing. MRI is more resource-intensive and less available than CT.
Overall, the staging accuracy of MRI in laryngeal cancer is slightly higher, largely because of more accurate assessment of cartilage involvement and paraglottic pre-epiglottic extension of tumor. CT is still more commonly used compared with MRI for initial staging of laryngeal cancer because of practical advantages, such as cost, speed, and availability.
Positron emission tomography–CT
Studies with sufficiently large numbers of patients investigating the role of positron emission tomography (PET)–CT in staging of laryngeal cancer are lacking. Recent reports suggest that PET evaluation of head and neck cancers may not present sufficient sensitivity or specificity to justify its routine use at the time of initial diagnosis , whereas others have reported that it significantly altered treatment in a substantial number of patients . Given the intrinsic limitation of spatial resolution of PET examination and its inability to assess lesions of small volume adequately, it would be unrealistic to expect that PET would improve T-staging of laryngeal cancer compared with clinical examination and CT or MRI. The accuracy of N-staging by PET is superior to other methods; however, currently, the negative predictive value of PET in nodal metastasis assessment is not sufficiently high to justify a change in treatment. PET has a distinct advantage compared with CT or MRI for detection of distant metastasis and should be routinely performed in patients with high risk for distant metastasis or when the primary site of neoplasm is unknown . It is possible that future development of more specific tracers or other improvements in technology may remedy some of these limitations. The role of PET-CT in posttreatment follow-up is well established by comparison, and PET-CT at the time of diagnosis may still provide a useful baseline for further management in some cases. Furthermore, PET imaging may be used to facilitate radiotherapy planning, which may provide sufficient justification for performing PET-CT at the time of initial imaging.
Choosing modality of imaging
CT versus MRI
State-of-the-art multichannel CT affords high spatial resolution images that can be reformatted in any desired plane, essentially negating the traditional advantage of MRI because of its multiplanar capability. Superior contrast resolution and multiparametric imaging (eg, T1-weighted, T2-weighted) remain significant advantages of MRI.
CT evaluation is much faster than MRI, substantially reducing or eliminating artifacts of movement attributable to breathing, swallowing, or coughing. MRI is more resource-intensive and less available than CT.
Overall, the staging accuracy of MRI in laryngeal cancer is slightly higher, largely because of more accurate assessment of cartilage involvement and paraglottic pre-epiglottic extension of tumor. CT is still more commonly used compared with MRI for initial staging of laryngeal cancer because of practical advantages, such as cost, speed, and availability.
Positron emission tomography–CT
Studies with sufficiently large numbers of patients investigating the role of positron emission tomography (PET)–CT in staging of laryngeal cancer are lacking. Recent reports suggest that PET evaluation of head and neck cancers may not present sufficient sensitivity or specificity to justify its routine use at the time of initial diagnosis , whereas others have reported that it significantly altered treatment in a substantial number of patients . Given the intrinsic limitation of spatial resolution of PET examination and its inability to assess lesions of small volume adequately, it would be unrealistic to expect that PET would improve T-staging of laryngeal cancer compared with clinical examination and CT or MRI. The accuracy of N-staging by PET is superior to other methods; however, currently, the negative predictive value of PET in nodal metastasis assessment is not sufficiently high to justify a change in treatment. PET has a distinct advantage compared with CT or MRI for detection of distant metastasis and should be routinely performed in patients with high risk for distant metastasis or when the primary site of neoplasm is unknown . It is possible that future development of more specific tracers or other improvements in technology may remedy some of these limitations. The role of PET-CT in posttreatment follow-up is well established by comparison, and PET-CT at the time of diagnosis may still provide a useful baseline for further management in some cases. Furthermore, PET imaging may be used to facilitate radiotherapy planning, which may provide sufficient justification for performing PET-CT at the time of initial imaging.
Malignant lesions of the larynx and staging
Supraglottis
The supraglottis is divided for the purposes of staging into several subsites: suprahyoid epiglottis, infrahyoid epiglottis, laryngeal surface of aryepiglottic folds, arytenoids, and false vocal cords. Nodal metastasis to levels II to IV is frequently seen. Essential imaging features include vocal cord fixation; tumor volume; and pre-epiglottic, paraglottic, and transglottic spread of disease.
T1: Tumor is confined to the site of origin, involving one supraglottic subsite. There is normal vocal cord mobility.
T2: Tumor extends to adjacent portions of the supraglottis or glottis (or adjacent extralaryngeal site, such as mucosa of the tongue base, vallecula, or medial wall of the piriform sinus). There is normal vocal cord mobility.
T3: There is vocal cord fixation or involvement of the pre-epiglottic space, paraglottic space, or inner cortex of the cartilages.
T4:
T4a: Tumor invades through the thyroid cartilage or invades tissues beyond the larynx.
T4b: Tumor invades the prevertebral space, encases the carotid artery, or invades mediastinal structures.
Glottis
T1: Tumor is confined to the vocal fold. The vocal fold retains normal mobility.
T1a: Involvement of a single vocal fold
T1b: Involvement of both vocal folds
T2: Tumor extends superiorly into the supraglottis or inferiorly into the subglottic region, or vocal cord mobility is altered.
T3: The vocal cords are fixed; however, tumor is confined to the larynx. The paraglottic space and the inner cortex of the cartilages may be involved,
T4:
T4a: Tumor invades through the thyroid cartilage or invades tissues beyond the larynx.
T4b: Tumor invades the prevertebral space, encases the carotid artery, or invades mediastinal structures.
Subglottic larynx
An isolated subglottic neoplasm is uncommon. Nodal drainage from this region includes level IV and level VI lymph nodes and the upper mediastinal lymph nodes.
T1: Tumor is confined to the subglottis.
T2: Tumor extends to the vocal folds.
T3: There is vocal cord fixation, but tumor remains confined to the larynx.
T4:
T4a: Tumor invades through the thyroid cartilage or invades tissues beyond the larynx.
T4b: Tumor invades the prevertebral space, encases the carotid artery, or invades mediastinal structures.
Pre-epiglottic and paraglottic space invasion
The pre-epiglottic space is situated between the epiglottis anteriorly and the hyoid bone, thyrohyoid membrane, and thyroid cartilage anteriorly. The pre-epiglottic space is readily identified on noncontrast T1-weighted MRI or CT, particularly in the sagittal plane, because of its largely fatty contents. On either side, the pre-epiglottic space is continuous with the paraglottic space (also known as the paralaryngeal space). The paraglottic space spans between the thyrohyoid membrane, thyroid and cricoid cartilages laterally and between the false and true vocal cords and the elastic cone medially. It contains fat at the level of the false vocal cords. This can be easily identified on axial and sagittal noncontrast T1-weighted MRI and CT, because fat tissue has unique imaging features. Invasion of the pre-epiglottic fat by glottic or supraglottic carcinomas is difficult to appreciate on clinical examination but is often readily appreciated by the head and neck radiologist as replacement of the normal fat on CT or MRI ( Figs. 3–5 ) . Likewise, imaging detection of paraglottic space involvement is reliable.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


