The authors present the clinical application of robotics to laryngeal surgery in terms of enhancement of surgical precision and performance of other minimally invasive procedures not feasible with current instrumentation. Presented in this article are comparisons of human arm with robotic arm in terms of degrees of freedom and discussion of surgeries and outcomes with use of the robotic arm. Robotic equipment for laryngeal surgery has the potential to overcome many of the limitations of endolaryngeal procedures by improving optics, increasing instrument degrees of freedom, and modulating tremor. Outside of laryngology, a multi-armed robotic system would have utility in microvascular surgery, procedures at the base of the skull, sinus surgery, and single-port gastrointestinal and thoracic access surgery.
The anatomy of the upper airway lends difficulty to the surgical treatment of laryngeal disease. Open surgery of the larynx allows for increased exposure of the surgical field and dexterity of instrumentation; however, healthy tissue, especially the delicate vibratory tissues and framework of the larynx, may be damaged during the procedure. In contrast, endoscopic laryngeal surgery uses natural body openings and therefore minimizes resultant damage to the framework. Even with advancements over the past 30 years, endoscopic laryngeal surgery continues to have disadvantages, including the operator’s distance from the surgical field, the laryngoscope’s relatively small exposure, and reduced depth perception with binocular vision. The lack of steerable modular instrumentation and three-dimensional (3D) viewing further handicap the laryngologist’s distal dexterity and suturing ability . Minimally invasive robotic surgery has the potential to address the shortcomings of endolaryngeal surgery and to significantly advance laryngeal surgery.
Endoscopic laryngeal surgery reduced invasiveness and improved outcomes since its introduction almost 100 years ago. In 1915, Lynch first reported the use of a laryngoscope for excision of glottic cancer. Lynch’s use of suspension laryngoscopy allowed for bimanual operation of instruments. Four decades later, Rosemarie Albrecht reported the addition of microscopy to enhance visualization of the larynx . Jako and Kleinsasser further refined laryngeal microsurgery by providing depth perception with binocular vision. Instrumentation evolved along with this new operative approach as microlaryngeal scissors, graspers, grippers, mirrors, elevators and suction devices were designed. The next development arrived in the early 1970s, when Jako and Strong combined the carbon dioxide laser with the operating microscope to provide for precise cutting and cauterization. Since then, lasers have been further refined with the microspot laser and microlaryngeal instruments have been further miniaturized. The powered microdebrider has been added to the armamentarium to lessen the operative time of and thermal damage caused by the laser .
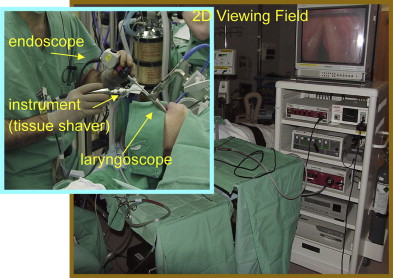
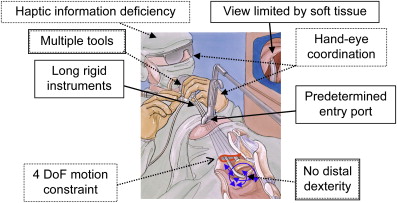
Other than miniaturization and the introduction of a few powered instruments, endolaryngeal surgery has evolved little in the past 30 years. The typical operative arrays employ either a handheld endoscope with one free hand to manipulate an instrument or the use of a binocular microscope that provides two hands to manipulate instruments ( Fig. 1 ). With either arrangement, the laryngoscope predetermines the port of instrument entry and provides a confined space that leads to instrument collision and often an obstructed view ( Fig. 2 ). Laryngologists remain restricted by the operator’s distance from the surgical field, the laryngoscope’s relatively small exposure, and reduced depth perception with binocular vision. These combine to restrict the surgeon’s ability to manipulate instruments across the long distance from the oral cavity to the larynx, resulting in poor sensory feedback (both visual and tactile) and magnification of operator tremor. Additionally, the lack of distal dexterity often causes damage to surrounding healthy tissue and limits surgical wound healing. While Woo and colleagues established endolaryngeal suturing techniques, suture repair of vocal fold wounds remains challenging due to technical complexities and the resulting increase in operative time . Suturing limitations result in larger scar formation. Fleming and colleagues demonstrated a 75% larger scar area when laryngeal defects healed with secondary intention versus primary intention. Larger vocal fold scars translate into worse voice outcomes. At this time, endoscopic laryngeal surgery has reached an impasse as the lack of distal instrument mobility, complexity of suture technique, and poor 3D vision limit surgical techniques that are routine in other surgical subspecialties.
Robotic equipment for laryngeal surgery has the potential to overcome many of the limitations of endolaryngeal procedures by improving optics, increasing instrument degrees of freedom, and modulating tremor. Currently, robotic surgery is employed in various specialties and in some cases has become the preferred procedure. The most commonly used system is the da Vinci Surgical Robot (Intuitive Surgical Inc, Sunnyvale, California), which is available at more than 170 hospitals throughout the United States . The da Vinci system was approved by the Food and Drug Administration (FDA) for general laparoscopic surgery in 2000 and thoracoscopy in 2001 . Robotic surgery has been employed in urologic surgery and gynecologic surgery, as well as to perform cardiac valve repair and coronary artery bypass grafting . The da Vinci Surgical Robot incorporates independently steerable arms and 3D imaging into a surgical cart and surgeon’s console. The surgeon’s console provides control of instrument arms with master robot manipulators. The surgical cart contains the slave robotic manipulators consisting of three arms: one to handle the endoscopic camera with the other two arms holding either two 8-mm (conventional adult size) or two 5-mm (pediatric size) endowrist instruments with increased distal freedom of motion. The 12-mm stereoscopic endoscope is equipped with two three-chip cameras that feed separate right and left views back to the vision cart, which creates a 3D perspective for the surgeon with separate monitors for right eye and left eye vision. Although its optics and tremor filtration represent key advances, the da Vinci Surgical Robot’s freedom of motion provides the greatest contribution to the surgical armamentarium.
The human arm represents the greatest actuator known to humans and represents the basis for which robotic surgical manipulators are constructed. The human arm is considered to have seven degrees of freedom provided by three joints. Degrees of freedom (DoF) are often described using nautical terminology such as pitch (tilting in a vertical vector), yaw (turning to the left or right), and roll (tilting from side to side). The shoulder is capable of pitch, yaw, and roll, the elbow pitch, and the wrist pitch, yaw and roll, totaling seven DoF. The elbow actuator of the human arm breaks the connection between the shoulder and wrist allowing for roll at both joints. That differs substantially from an endolaryngeal instrument being manipulated by a human arm or the da Vinci surgical robot effector arm. Endolaryngeal instruments are limited by their straight shaft, lack of a wrist actuator, and the small opening of the laryngoscope. When operated by the human hand, endolaryngeal instruments have four DoF: the yaw, pitch, and roll of the human hand and the ability to move in an out. The degrees of yaw and pitch are limited by the laryngoscope’s opening. When compared with the human arm, the da Vinci surgical robot has six DoF. The unique isocenter of motion-proximal actuator allows each robotic arm to pivot around a point outside of the volume of the actuator. That is usually at the point of insertion into the human body, which would be the equivalent of the shoulder in a human arm analogy. However, because the robotic arm is a straight shaft (lacking the elbow of the human arm), the roll at the point of skin insertion is the same roll at the endowrist joint. Therefore, the six DoF of each da Vinci slave manipulator are from yaw and pitch at the endowrist and skin insertion point, roll along the shaft, and the ability to move in and out of the port. These six DoF allow for comparable tissue manipulation to that of the human arm during open surgical procedures and its application has the potential to greatly advance laryngeal surgery.
The enthusiasm for applications of robotic surgery in otolaryngology–head and neck surgery have been slowed by ease of access to body orifices and the relative ease of hiding surgical wounds out of the line of site in the hairline or in mucous membranes. Applications in laryngeal robotic surgery have been further limited by the endotracheal tube in the operative field and manipulation of the robotic instrument arms in the narrow oral, pharyngeal, and laryngeal spaces . Furthermore, the da Vinci Surgical Robot was designed for opposing arms inserted via widely spaced ports of entry in the abdomen and thorax. These applications are quite different from the need for parallel ports of entry through the narrow opening of a laryngoscope.
In 2005, McLeod and Melder were the first to report use of the da Vinci Surgical Robot in laryngeal surgery, performing a robotic-assisted excision of a vallecular cyst. The authors used a slotted laryngoscope, which only provided operative space for one 8-mm robotic arm in addition to the 12-mm stereoscopic camera. A surgeon assisted on the case by providing olive tip tissue countertraction. The robot’s arm successfully marsupialized the cyst with round-tip cautery, procured biopsies of the cyst wall, and placed oxymetazoline-soaked pledgets for hemostasis. The procedure was performed without complication and the patient was discharged the same day. The total case time was 109 minutes, however 89 minutes were spent setting up the robot. The authors concluded that superb 3D visualization allowed for accurate assessment and precise instrument control . While it was feasible to use the robot in the human airway, the laryngoscope provided limited space for operative maneuvering.
The volume limitations of the laryngoscope were overcome with the use of a mouth gag to retract the mouth tongue and cheeks. Hockstein and colleagues reported the technical feasibility of operating with the three arms of the da Vinci Surgical Robot through a Dingman mouth gag for airway surgery on a mannequin and cadavers. The Dingman mouth gag with cheek retractors achieved satisfactory exposure, unimpeded instrument movement, precise handling of tissue, and an ability to perform endolaryngeal suturing. Initial experiments focused on various pharyngeal and microlaryngeal procedures, including arytenoidectomy, partial epiglottectomy, and partial resection of the base of tongue to demonstrate efficacy with the robot. In each procedure the tongue was retracted, a 30-degree upward-facing endoscope was used for visualization, and both 5-mm and 8-mm diameter instruments were used. The duration of each procedure was comparable to conventional operative methods. Furthermore, Hockstein and colleagues reported an increase in freedom of instrument mobility, improved depth perception with the 3D imaging, scaling of movement (from the large movement of the operator’s hand to the small movement of instrument), and removal of tremor. Last, Hockstein and colleagues concluded that the safety profile of transoral robotic surgery was comparable to that of conventional endoscopic laryngeal surgery.
Success with cadaveric robotic surgery has translated into clinical experimentation with the da Vinci Surgical Robot, including published reports of transoral robotic supraglottic partial laryngectomy and base of tongue neoplasm resection . Preclinical studies animal studies preceded each clinical study of three patients . Both studies used 8-mm instrumentation with visualization by 0° and 30° high magnification endoscopes through FK mouth retractors. These studies introduced the use of electrocautery robotic instruments and a flexible tracheal suction device manipulated by a robotic arm . A surgeon assisted each robotic procedure with the application of surgical clips. The mean surgical time for supraglottic transoral robotic surgery was 120 minutes, while the base of tongue procedures averaged 105 minutes . These results included robotic positioning and exposure, however the results omitted set-up time. The six procedures in both studies were completed robotically without complication and with minimal blood loss . The authors concluded that base of tongue neoplasm excision and supraglottic laryngectomy were technically feasible and safe with the da Vinci Surgical Robot, allowing for good exposure and complete tumor resection.
In a separate study, Rahbar and colleagues described success using the da Vinci Surgical Robot in pediatric airway surgery to repair laryngeal clefts in five patients. Before the introduction of the robot, a carbon dioxide laser was used to denude the mucosal margin of the cleft. A Crowe-Davis mouth gag provided sufficient exposure to employ both a 0° and 30° endoscope, with the 30° endoscope providing superior exposure of the glottis. The authors described restricted movement with both 5-mm and 8-mm-diameter instruments. Ultimately, inadequate surgical access resulted in abandoning the robotic approach in three patients. In the other two patients, transoral robotic repair was successful as defined by endolaryngeal suturing to close the cleft . In these cases, robotic operative time was increased by an average of 40 minutes as compared with routine endoscopic approach .
Robotic surgery has clear advantages in motor control and visualization when compared with conventional endoscopic laryngeal surgery. The da Vinci Surgical Robot’s 3D optics system creates a superb wide-view high-definition illusion of a 3D surgical field. Its movable endoscope expands the surgical field by changing viewing angles and position translating to greater surgical precision. Motor control is improved with a combination of movement scaling, tremor modulation, and increased instrument freedom of motion. The da Vinci master-slave robotic manipulators filter out natural hand tremor, adjust the large hand movements of the operator to the small movements of instruments in the airway, and enhance dexterity, to allow for more precise instrument movement and prevent instrument collision within the airway . Instrument control is further enhanced with distal articulation by the da Vinci’s endowrist design, providing flexion, extension, pronation, and supination at the distal end of instruments for finer tissue manipulation.
In comparison to transoral laser surgery, robotic surgery’s rotational optics is superior to line-of-sight visualization with the operating microscope. Furthermore, the robotic arms allow for en bloc tumor resection as opposed to the piecemeal cutting of the tumor with the laser . Finally, robotic airway surgery allows for certain procedures that are more commonly performed with an open approach, such as excision of supraglottic or base of tongue cancer, to be successfully completed through an endoscope. This decreases morbidity to adjacent tissue and bony structures associated with open procedures and precludes need for tracheostomy .
While the da Vinci Surgical Robot has advantages over open and endoscopic laryngeal surgery, there are limitations in its design. The current da Vinci robot was designed for abdominal and thoracic surgery with large-diameter instruments predicated on laparoscopic instruments. The arms of the robot were designed to mimic the opposition of a surgeon’s hands in conventional surgery; the robot arms were not designed to be coaxial with the lumen of a laryngoscope. The current 12-mm-diameter endoscope competes with space with 8-mm adult and 5-mm pediatric instruments. This is evidenced by McLeod and Melder’s inability to place both robotic arms within the laryngoscope during their robot-assisted excision of a vallecular cyst. They also reported a lengthy set-up process that took two-and-a-half times as long as the procedure itself . Last, their robot arms did not have a suction device, which was provided by a surgeon-assistant . While Weinstein and colleagues ultimately attached an endotracheal suction to a robotic arm, the current da Vinci robot lacks an integrated suction device . While all three robotic arms fit through the mouth gag, both Hockstein and colleagues and Rahbar and colleagues reported limited access resulting in instrument crowding. Instrument crowding is partially responsible for the challenges of suturing with the da Vinci Surgical Robot in the airway. The primary reason is the limited distal dexterity of the instruments, which lack the ability to roll, the key motion in passing a curved needle. Rahbar and colleagues were able to suture two laryngeal clefts, albeit with the endosuture technique. Additionally, because of the robotic arm opposition, the procedure is performed with a wide angle between instruments resulting in a technically complex and awkward operation. Last, the $1.5 million initial cost and $100,000 annual service contract for the da Vinci Surgical Robot make it prohibitive for hospitals to acquire solely for airway procedures . For the da Vinci system to be cost efficient, otolaryngologists likely will have to be at large hospitals that have purchased a robot for urologic, cardiothoracic, laparoscopic, and gynecologic applications .
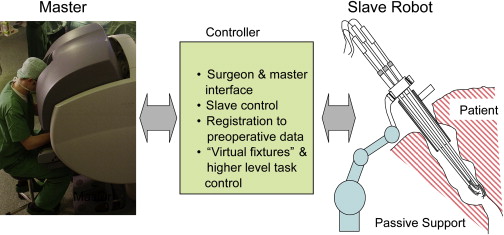
Further advancements in robotic surgery are necessary to facilitate the entry of robotic surgery into the otolaryngologist’s armamentarium. Future prototypes will incorporate instrument miniaturization, robot arms that function in the coaxial plane of the laryngoscope, integration of suction and powered instruments into the robots arms, and enhanced tool-tip dexterity. Our laboratory is developing a modular, scalable surgical robot to address the limitations of the current da Vinci Surgical Robot for applications in the airway ( Fig. 3 ). A prototype has been designed with 4-mm-diameter snakelike instrument arms ( Fig. 4 ). The snakelike arms are able to enter the laryngoscope in near parallel position and are designed with continuous backbones rather than pins or joints ( Fig. 5 ). This central backbone design designed has the potential to deliver a variety of instruments including a laser, suction, drill, and other powered instruments. The arms are controlled by compact tool manipulation units at the proximal end well outside of the field of surgery. Enhanced tool-tip dexterity (distal dexterity) is provided with a flexible snakelike motion as compared with the articulating endowrist design of the da Vinci Robot. The increased distal flexibility improves the robot’s ability to maneuver in the small operative space of the airway, enabling suturing and functional reconstruction of tissue ( Fig. 6 ). The snakelike robot is specialized for minimally invasive surgery of the airway and is not modeled after the human arm. The small arm size and unique motion of robotic arms is designed to use less volume of motion to perform a surgical task. Each robotic arm has two snakelike units that may be compared with the curve of a finger. Each robotic arm has eight DoF with the proximal actuators capable of moving up and down, moving right and left, moving in and out, and roll. Furthermore, each of the two snakelike units within the arm is capable of yaw and pitch.