Purpose
To distinguish differences in retinal nerve fiber layer (RNFL) thickness and peripapillary total retinal volume between eyes with papilledema, pseudopapilledema, and normal findings.
Design
Cohort study.
Methods
Forty-two eyes with mild papilledema, 37 eyes with congenitally elevated optic disc (pseudopapilledema), and 34 normal eyes met the inclusion criteria at 1 academic institution (in Iran) and underwent neuro-ophthalmic examination. Spectral-domain optical coherence tomography scans surrounding the optic disc were performed in each eye of patients and subjects. Main outcome measures were mean RNFL thickness and peripapillary total retinal volume measurements (inner and outer ring volumes) that were compared between groups, using the generalized estimating equation approach. Area under receiver operating characteristic curves were also calculated.
Results
A statistically significant difference was found in mean RNFL thickness between both groups of patients with papilledema and pseudopapilledema and normal subjects. Average inner peripapillary total retinal volume in the papilledema, pseudopapilledema, and control groups were 1.95 ± 0.24 mm 3 , 1.81 ± 0.23 mm 3 , and 1.06 ± 0.10 mm 3 , respectively. Average outer peripapillary total retinal volume in the papilledema and pseudopapilledema groups were 2.68 ± 0.49 mm 3 and 2.03 ± 0.24 mm 3 , respectively ( P < .001). However, the outer ring peripapillary total retinal volume was not different between pseudopapilledema and normal (1.90 ± 0.11 mm 3 ) eyes ( P = .17). Area under the curve to discriminate pseudopapilledema vs papilledema eyes for average RNFL thickness and inner and outer peripapillary total retinal volumes was 0.82, 0.68, and 0.88, respectively.
Conclusion
Outer peripapillary total retinal ring volumes might be useful in differentiating papilledema from pseudopapilledema.
Papilledema is observed as optic disc swelling and results from axonal stasis secondary to raised intracranial pressure. It is important to consider pseudopapilledema caused by congenital optic disc elevation or optic disc drusen in the differential diagnosis of mild to moderate optic disc swelling. Although there may be ophthalmoscopic clues that allow identification of anomalous optic disc elevation (such as drusen, anomalous surface vessels, and clear peripapillary nerve fiber layer), mild to moderate papilledema cannot be distinguished reliably ophthalmoscopically from pseudopapilledema. Several studies have attempted to use optical coherence tomography (OCT) to differentiate these 2 conditions. OCT can show optic nerve head drusen or retinal nerve fiber thinning. However, in those individuals with congenitally elevated optic discs, OCT shows increased thickness of the peripapillary retinal nerve fiber layer (RNFL), similar to that which occurs in mild papilledema. Several groups have shown that peripapillary subretinal fluid may be seen exclusively in patients with true disc edema (in contrast to pseudopapilledema) and calculated 2-dimensional (2-D) peripapillary total retinal thickness. Peripapillary assessment is appropriate because papilledema manifests as swelling of the peripapillary retina and optic nerve. However, 2-D OCT is subject to artifact because of the variable thickness caused by the edema, and this result may distort the findings. In addition, it is difficult to quantify the papilledema (a volumetric parameter) without using 3-dimensional (3-D) images.
Spectral-domain OCT forms 3-D maps of the retina and optic nerve and is able to produce true volumetric image data, using raster scanning. Three-dimensional optic nerve head morphology has been quantified in patients with glaucoma and papilledema by segmentation of OCT scans. More recently, a peripapillary total retinal volume centered at the optic nerve head has been introduced in the Spectralis OCT (Heidelberg Engineering, Heidelberg, Germany), which provides the ability to quantify volumetrically the optic disc swelling. Consequently, we investigated the potential benefit of quantitative differences in RNFL thickness and peripapillary total retinal volume in differentiating pseudopapilledema caused by congenital optic disc elevation from papilledema on commercial SD OCT software.
Methods
Patients and Participants
This was a longitudinal, comparative/cohort study conducted in the neuro-ophthalmology service of Farabi Eye Hospital, Tehran. The study was approved by the local ethics committee of the Tehran University of Medical Science and was conducted in accordance with the Declaration of Helsinki. All participants gave written informed consent.
Patients referred to the Farabi Eye Hospital neuro-ophthalmology clinic between September 2010 and February 2013 for “presumed papilledema” in the acute phase were eligible. Each patient underwent ophthalmologic examination, including refractive assessment, afferent pupillary light reflex testing, slit-lamp examination, intraocular pressure measurement, funduscopy, automated perimetry, OCT examination, and ocular B-scan ultrasound. Additional neuroradiologic studies (brain magnetic resonance imaging and magnetic resonance venography) and lumbar puncture (cerebrospinal fluid pressure measurements and cerebrospinal fluid composition) were obtained in selected subjects.
Among 81 subjects consecutively referred for presumed papilledema, definitive diagnoses were achieved in 72. Patients with optic disc drusen visible by ophthalmoscopy, OCT, or B-scan (n = 15), moderate to severe (Frisén grade 3–5) papilledema (n = 9), atrophic papilledema (n = 2), and previous retinal disease (n = 1) were excluded from further study. This left 45 patients with either mild papilledema (n = 24) or congenitally elevated optic discs (n = 21).
A group of age- and sex-matched controls (n = 19) without symptoms of increased intracranial pressure was recruited among employees. All had best-corrected visual acuities of at least 20/20, normal visual fields, and no optic nerve head abnormalities.
Optical Coherence Tomography
RNFL thickness and 3-D peripapillary total retinal volume scans were obtained using SD OCT (Heidelberg Spectralis SD OCT; Heidelberg Engineering; Spectralis software version 5.3.2) for each eye of the patients and controls. RNFL thickness was measured using a 3.4-mm circular scan around the optic nerve head. Peripapillary total retinal volume was measured by a raster scan protocol, which generated 73 slices (B-scans) over a 4 × 4 × 2 mm 3 volume centered on the optic nerve head with a scanning angle of 15 × 15 degrees and a resolution of 384 A-scans per B-scan. The peripapillary total retinal volume was defined by the volumetric region (in mm 3 ) between the segmented inner limiting membrane and the lower bounding reference surface of the retinal pigment epithelial complex in a cube using the device software’s segmentation algorithm. Circular lines on the cube represent 1-, 2.2-, and 3.45-mm scan diameter ( Figure 1 ). The innermost circle (1 mm) volumes’ data were ignored because they fell inside the optic nerve area. Peripapillary total retinal volumes were calculated as volumes for ring-shaped areas between the 1-mm-diameter and 2.2-mm-diameter circles for the inner peripapillary total retinal volume and between the 2.2-mm-diameter and 3.45-mm-diameter circles for the outer peripapillary total retinal volume. These regions were also examined further in 4 quadrant volumes (superior, inferior, temporal, and nasal). Mean peripapillary total retinal thickness was also calculated by the software. However, we did not use the thickness values. A real-time eye tracker couples the SD OCT scanner to the eye position and stabilizes the OCT scan on the retina. All testing was carried out by the same operator (M.K.). Quality scores for scans are expressed as a signal-to noise ratio in decibels (dB). Scans above 20 dB were considered an acceptable quality.
In this study both (correlated) eyes of each subject were used in the analysis. If this within-cluster correlation is not accounted for in the analyses, parametric standard errors may be biased and application of some statistical tests will lead to erroneous statistical inferences. Therefore, generalized estimating equations were used to compare the average or quadrantic RNFL thickness and peripapillary total retinal volume measures in each group. We used these methods to extend the generalized linear model and to allow for analysis of correlated observations, such as clustered data. The main advantage of generalized estimating equations resides in the consistent estimation of parametric standard errors. Receiver operating characteristic curves were used to describe the sensitivity and specificity of each variable to differentiate pseudopapilledema from papilledema. Areas under the receiver operating characteristic curve (AUCs) and comparison between AUC values were also measured. ROCKit software was used to calculate AUC values and the other statistical analyses were carried out using Stata software version 11.0 (StataCorp, College Station, Texas, USA). Differences were significant at P < .05.
Results
For all analyses involving OCT measurements, OCT data of 7 of 64 patients (11%) were excluded because of poor software segmentation. Therefore, data of 21 patients with papilledema (n = 42 eyes) and 19 with pseudopapilledema (n = 37 eyes) and 17 normal subjects (n = 34 eyes) were analyzed. From 21 patients with papilledema, 10 had Frisén grade 1 and 11 had Frisén grade 2, with grading agreement between 2 experts on independent examination. This group consisted of 17 patients with idiopathic intracranial hypertension and 4 patients with intracranial hypertension secondary to cerebral venous sinus thrombosis; all had lumbar punctures showing intracranial pressure of more than 200 mm H2O. Of the 19 patients determined to have pseudopapilledema, 16 had intracranial pressure measurements of less than 200 mm H2O. The other 3 (including 1 patient with unilateral disc elevation) had stable optic nerve appearance during follow-up, with no signs or symptoms for increased intracranial pressure, and thus did not have a lumbar puncture performed.
Mean best-corrected visual acuity was 0.03 ± 0.05 logMAR and 0.04 ± 0.04 logMAR in the pseudopapilledema and papilledema groups, respectively. Automated visual field tests demonstrated mild defects (superior and/or inferior arcuate, enlarged blind spot, or generalized depression) for 26 of the 37 eyes (70%) in the pseudopapilledema group (average mean deviation, −1.7 ± 2.1 dB) and for 39 of 42 eyes (93%) in the papilledema group (average mean deviation, −4.3 ± 2.7 dB). The most common visual filed defects were arcuate visual field loss (15 eyes) and enlargement of the blind spot (20 eyes) in pseudopapilledema and papilledema groups, respectively.
Retinal Nerve Fiber Layer Thickness Measurements
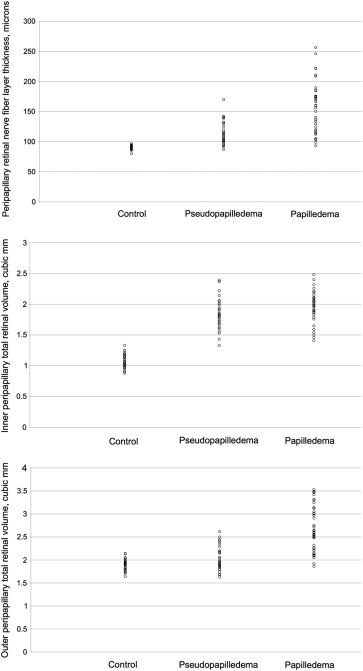
Average RNFL thickness in the papilledema, pseudopapilledema, and control groups was 156.3 ± 40.1 μm, 113.8 ± 18.7 μm, and 90.5 ± 3.1 μm, respectively. Average RNFL thickness values were significantly greater in the papilledema group than in the pseudopapilledema group (generalized estimating equation, P < .001). Similarly, average RNFL thickness values were significantly greater in the pseudopapilledema group than in the control group ( P = .001). In addition, RNFL thickness values were significantly greater in all quadrants in the papilledema group than in the pseudopapilledema (temporal, P = .001; other quadrants, P < .001). There were significant differences in RNFL thicknesses in the pseudopapilledema group vs the control group in 3 quadrants (superior, P = .004; inferior, P = .01; nasal, P = .03) ( Table 1 ); however, overlap among the groups also was observed ( Figure 1 , Top).
| Scanning Region | Parameter | Control Group (n = 34) | Pseudopapilledema Group (n = 37) | Papilledema Group (n = 42) | P a Value Control vs Pseudopapilledema | P a Value Pseudopapilledema vs Papilledema | P a Value Control vs Papilledema |
|---|---|---|---|---|---|---|---|
| RNFL (μm) | Average | 90.5 (3.1) | 113.8 (18.7) | 156.3 (40.1) | .001 | <.001 | <.001 |
| Superior | 115.4 (6.0) | 143.2 (35.3) | 177.9 (58.7) | .004 | <.001 | <.001 | |
| Inferior | 117.3 (6.1) | 146.8 (27.0) | 204.5 (61.7) | .013 | <.001 | <.001 | |
| Temporal | 63.2 (3.9) | 78.6 (13.8) | 108.0 (48.1) | .084 | .001 | <.001 | |
| Nasal | 66.0 (4.3) | 86.4 (25.1) | 135.0 (46.3) | .037 | <.001 | <.001 | |
| Peripapillary total retinal volume (mm 3 ) | Inner (total) | 1.06 (0.10) | 1.81 (0.23) | 1.95 (0.24) | <.001 | .013 | <.001 |
| Inner superior | 0.29 (0.02) | 0.47 (0.07) | 0.51 (0.06) | <.001 | .011 | <.001 | |
| Inner inferior | 0.28 (0.03) | 0.47 (0.08) | 0.51 (0.07) | <.001 | .016 | <.001 | |
| Inner temporal | 0.21 (0.03) | 0.40 (0.05) | 0.43 (0.08) | <.001 | .121 | <.001 | |
| Inner nasal | 0.27 (0.03) | 0.45 (0.06) | 0.48 (0.06) | <.001 | .056 | <.001 | |
| Outer (total) | 1.90 (0.11) | 2.04 (0.24) | 2.68 (0.49) | .172 | <.001 | <.001 | |
| Outer superior | 0.50 (0.03) | 0.53 (0.08) | 0.71 (0.15) | .463 | <.001 | <.001 | |
| Outer inferior | 0.50 (0.03) | 0.57 (0.07) | 0.76 (0.16) | .056 | <.001 | <.001 | |
| Outer temporal | 0.45 (0.02) | 0.47 (0.05) | 0.61 (0.12) | .284 | <.001 | <.001 | |
| Outer nasal | 0.43 (0.03) | 0.46 (0.06) | 0.59 (0.11) | .273 | <.001 | <.001 |
Peripapillary Total Retinal Volume Measurements
Average inner peripapillary total retinal volumes in the papilledema, pseudopapilledema, and control groups were 1.95 ± 0.24 mm 3 , 1.81 ± 0.23 mm 3 , and 1.06 ± 0.10 mm 3 , respectively. Average outer peripapillary total retinal volumes in the papilledema, pseudopapilledema, and control groups were 2.68 ± 0.49 mm 3 , 2.03 ± 0.24 mm 3 , and 1.90 ± 0.11 mm 3 , respectively ( Figure 1 , Middle and Bottom). Inner peripapillary total retinal volumes and all its quadrants’ volumes were greater in the papilledema ( P < .001) and pseudopapilledema ( P < .001) groups than in the control group. Although the superior and inferior quadrants’ inner peripapillary total retinal volumes were greater in the papilledema group vs the pseudopapilledema group (generalized estimating equation, all P < .001), a significant difference was not found between 2 groups in the temporal and nasal quadrant inner peripapillary total retinal volumes. On the other hand, neither the total nor any quadrantic outer peripapillary total retinal volumes were statistically different between pseudopapilledema and control groups. Additionally, eyes with papilledema, compared with the pseudopapilledema and control groups, showed significantly greater outer peripapillary total retinal volume in all quadrants (all P < .001) ( Table 1 ). Figures 2–4 show examples of RNFL thickness and peripapillary total retinal volume measurements in 1 subject from each of the 3 groups.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


