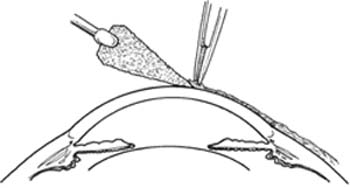
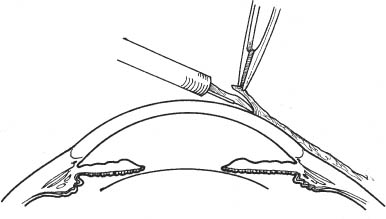
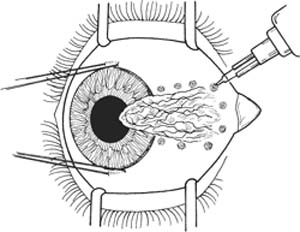
17 Note: the free conjunctival graft or amniotic membrane technique is preferred for treating advanced and recurrent pterygium. This technique has been shown to decrease the rate and severity of pterygium recurrence. The primary disadvantage of the graft technique is prolonged operative time. Treat any significant inflammation with topical steroids, as it is best to operate on the least inflamed tissue possible. Optional: Prophylactic antibiotics (see Chapter 3). Note: Primary bare sclera pterygium excision has a high recurrence rate. 1. Anesthesia: a. Topical anesthetic (e.g., proparacaine). b. Peribulbar or retrobulbar plus lid block in uncooperative patient or when surgical time is anticipated to be long. 2. Prep and drape. a. Use povidone-iodide 5% on a cotton-tipped applicator to gently clean eyelashes and lid margins. b. Place one or two drops of povidone-iodide in the conjunctival fornix. 3. Insert lid speculum. 4. Perform forced duction testing to rule out any restriction of rectus muscles secondary to involvement with the pterygium (0.3 forceps). 5. Optional: Place a double-armed 6–0 silk episcleral limbal stay suture at the 6 or 12 o’clock meridian, or both. 6. Position eye with stay sutures and clamp. Figure 17.1 7. Demarcate the body of the pterygium with cautery (Fig. 17.1). a. Place spots on normal conjunctiva along the area to be resected. b. Note: If administering subconjunctival lidocaine under the body of the pterygium, do so after placing demarcation spots. Figure 17.2 8. Use the tip of a dry cellulose sponge to bluntly undermine the head of the pterygium (the part on the cornea as opposed to the tail, which is on the sclera) while applying counter traction (lifting pterygium) with tissue forceps (Fig. 17.2). Note: Remove as much as the pterygium as possible from corneal surface using cellulose sponges. Sponges will need to be changed constantly. Figure 17.3 Alternatively, grasp the head of the pterygium using a 0.3 or 0.12 forceps and lift while using a Beaver #57 blade to perform a lamellar dissection (Fig. 17.3).
Pterygium Excision
Indications
 Reduced vision secondary to:
Reduced vision secondary to:
 Pterygium advancing toward or already impinging upon visual axis
Pterygium advancing toward or already impinging upon visual axis
 Induced astigmatism
Induced astigmatism
 Cosmesis
Cosmesis
 Significant discomfort that is not relieved by medical therapy
Significant discomfort that is not relieved by medical therapy
 Limited ocular motility secondary to muscle restriction
Limited ocular motility secondary to muscle restriction
Preoperative Procedure
Instrumentation
 Lid speculum (e.g., Lieberman or Barraquer)
Lid speculum (e.g., Lieberman or Barraquer)
 Bishop-Harmon forceps
Bishop-Harmon forceps
 Tissue forceps (e.g., 0.12 mm and 0.3 mm Castroviejo)
Tissue forceps (e.g., 0.12 mm and 0.3 mm Castroviejo)
 Anatomic forceps
Anatomic forceps
 Disposable cautery
Disposable cautery
 Sutures (6–0 silk, 10–0 nylon, 10–0 Vicryl)
Sutures (6–0 silk, 10–0 nylon, 10–0 Vicryl)
 Scarifier (e.g., Grieshaber #681.01 or Beaver #57)
Scarifier (e.g., Grieshaber #681.01 or Beaver #57)
 Cellulose sponges
Cellulose sponges
 Cotton-tipped applicators
Cotton-tipped applicators
 Westcott scissors
Westcott scissors
 Diamond burr
Diamond burr
 Castroviejo calipers
Castroviejo calipers
 Needle holder
Needle holder
 Clamp
Clamp
Operative Procedure
Bare Sclera Pterygium Excision
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


