Pterygium and Its Surgery
Gurinder Singh
DEFINITION
Pterygium (From the Greek pterygos, meaning “wing”; plural, “pterygia”) is a triangular, wing-shaped, degenerative, fibrovascular, hyperplastic proliferative tissue actively growing from the conjunctival limbal area onto the cornea (Fig. 60-1). Usually it is preceded by pinguecula (from the Latin pinguis, “fat”; plural, “pingueculae”), which itself is a degenerative tissue involving conjunctiva and underlying episclera. Pterygium is usually a raised leash of fibrovascular conjunctival tissue that grows very gradually onto cornea in the interpalpebral area. It continues to grow toward the center of the cornea, mostly from the nasal side, but it can come from the temporal side; it rarely grows from both nasal and temporal sides simultaneously.
HISTORY
According to Bidyadhar (1,2), Rosenthal (3), Thomas (4), and Jaros and DeLuise (5), the first recorded description of pterygium and the surgical procedure to treat it was by Susruta, the world’s first surgeon-ophthalmologist, who lived in India around 1000 B.C. Since then, Celsus (29 A.D.), Vagblat (third to fourth century), Paul (600 A.D.), Rhazes (932 A.D.), Avicenna (1037 A.D.), Chakradatta (1060 A.D.), and others have described it in detail (3,6). Almost all of these authors suggested surgical treatment for the condition with modifications to the original procedure recommended by Susruta.
Numerous practitioners, including Merigot de Teigny, Coirre, Aëtius, Hippocrates, Celsus, Galen, Archigenes, Saint-Yves, Maitre Jean, Desmarres, Gonin, and others, attempted medical treatment of pterygium. They tried various forms of collyrium of lead, zinc, copper, iron, bile, urine, women’s milk, white wine, vinegar, candied sugar, water of Euphrasia, cuttlefish bone, silver nitrate, lead acetate, mercuric lanoline, and others (3,4,6).
Similarly, many surgical procedures have been described, tried, and advocated since the time of Susruta. Many surgeons have warned of the dangers of the procedures, and have advised temporizing as long as vision was not impaired. Some have recommended surgery only if the patient was “esthetically tormented” (3). Celsus of Rome (around 1 A.D.) used a scalpel to remove pterygium from the cornea after lifting it from the sclera with a thread passed beneath it. Paul of Aegineta used horsehair to saw it from its attachments. Ali bin Isa, of Baghdad, recognized two types of pterygia, and recommended surgery only for the hard, red type and not for the soft, delicate type (3). Ali bin Isa recommended putting the patient to sleep for the surgery, which suggests that Arabs may have been the first to use general anesthesia. Acrel (1771) was the first to perform total removal of the head of pterygium from the cornea and circumscribe it with the bistoury (3).
It seems that Scarpa in 1802 was the first to perform a kind of bare-sclera excision of pterygium, later performed by Travers (1805), Westhoff, Peterquin, Pellier de Opinsy, and Rubio. Bell (1813), Woolhouse, and Beer recommended cauterization and scarification of the pterygium. Grandelement used chromic acid, McCallan used carbonic snow, Ajily-Bay-Haydar used silver nitrate, and Shaugnessy used nitric acid to treat pterygia (3). Coccius, and later Arlt, successfully closed the conjunctival resection bare-sclera area with sutures in an attempt to prevent recurrence of the pterygium. Weller (1832) and Walton (1853) transfixed the neck of the pterygium with a thread passed underneath, and then cut the corneal attachment and the base of the growth, extirpating the growth. Arlt (1850) removed a rhomboid of tissue and closed the wound in a cruciate manner (3).
The elder Desmarres (7) devised the procedure of transplantation of the pterygium for the purpose of diverting the growth from the cornea into the adjacent lower fornix. He mobilized a small flap of conjunctiva that was sutured between the mobilized pterygium and the corneal margin. The pterygium atrophied after this procedure, and that established a principle used in all transplantation operations. Terrien brought the pterygium growth upward to the upper fornix. Knapp (1868) bisected the growth and pulled the upper half superiorly and the lower half inferiorly. Hobbs (1894) introduced the use of galvanocautery
(52 V) for cutting across the neck of the pterygium, and Coe (1896) and Loring advocated the use of thermal cautery with a heated platinum wire (3).
(52 V) for cutting across the neck of the pterygium, and Coe (1896) and Loring advocated the use of thermal cautery with a heated platinum wire (3).
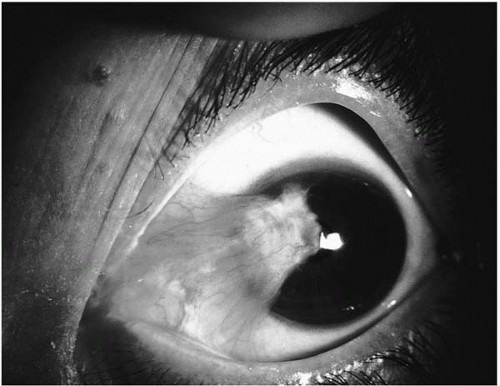 FIGURE 60-1. Primary nasal pterygium growing into visual axis.(see color image) |
Free tissue grafts to cover the bare sclera after pterygium excision were introduced by Klein in 1876. He used mucous membrane grafts in cases in which insufficient bulbar conjunctiva was left after pterygium excision to cover bare sclera (3). Gifford (1909), Cozalis (1920), Duverger (1926), Green (1937), and Dosorova (1942) also used these grafts. In 1888, Hobby mobilized adjacent conjunctiva to cover bare sclera. Elschnig covered the bare sclera with a pedicle conjunctival flap graft. Hotz (1892) used the Thiersh grafts with success (3). Gifford used these grafts in recurrent pterygia. Autografting with free fragments of conjunctiva was used by de Gama Pinto, Gomez-Marques, and de Paula Xavier. In 1931, Mata covered the denuded area after pterygium excision with buccal mucous membrane (8). Hawley, in 1911, introduced the use of superficial thin skin grafts from behind the ear or from the thigh, and reaffirmed his procedure in 1937 (9,10). Morax and Magitot, in 1911, tried the use of artificially preserved homografts from the corneas of fetuses and adults, the early forms of corneal grafting. Terson of Paris first referred to the use of radiation treatment after pterygium excision in 1911(11). Burnam and Neill, in 1940, described their use of radon to prevent pterygium recurrence. Since then, Ruedemann, Iliff, Swanberg, Hughes, and many others have used radium, radon, and beta irradiation as adjunctive treatment to pterygium excision (3).
The procedure of “subvolution” was devised by Galezowski in 1880, tried by Numar, and named by Bettman in 1894 (12). It involved freeing the head and neck of the pterygium and folding it under the body of the pterygium and suturing the edges. Avulsion of a pterygium head from the cornea with a muscle hook occurred accidentally while Prince in 1885 was performing another procedure. A similar accident happened to Wright in 1888. Wright has recorded a case of a patient who pulled his own pterygium from his cornea with “eye tweezers,” without anesthesia, and with excellent results (3). Boeckman, in 1885, suggested recession of conjunctival edges after excision of the head to the pterygium and suturing the conjunctival edges to their new position, leaving behind bare sclera to reepithelialize by itself (13).
Rosenthal has concluded his article on the chronology of pterygium therapy by saying
down through history were many who practiced and reported upon various operative techniques without making any outstanding contributions. They number in hundreds and their names may be found in the literature of all nations and all ages. And so it appears that for about 30 centuries man has tried to conquer this little growth called pterygium. It had been incised, removed, split, transplanted, excised, cauterized, grafted, inverted, galvanized, heated, dissected, rotated, coagulated, repositioned, and irradiated. It has been analyzed statistically, geographically, etiologically, microscopically, and chemically—yet it grows onward primarily and secondarily. We look with interest to its future (3).
With this background, I venture to discuss what is known about pterygium and its current treatment.
EPIDEMIOLOGY
Geographic Distribution
The prevalence of pterygium has been directly related with proximity to the equator: the nearer to the equator, the greater the prevalence. Most commonly seen on either side of the equator, pterygium has been endemic in the Indian subcontinent, Southeast Asia, Hawaii, the Samoan Islands, the Middle East, Mexico, the Caribbean, Australia, Northern and Western Africa, and the sunbelt states of the United States. Cameron’s world map summarizes the prevalence rates of pterygium (14). Generally rare in the cooler climates of Europe and the northern states in the United States, its prevalence, oddly, is high among the Inuit (Eskimos).
Prevalence
Prevalence rates of pterygium have been as high as 22.5% on the island of Aruba (15 degrees latitude from the equator), 18% in Puerto Rico (18 degrees latitude), and 5% to 15% in Texas, Florida, California, Arizona, and New Mexico in the United States (latitude 28 to 36 degrees from the equator). The prevalence rate drops to 2% or less in geographic areas more than 40 degrees from the equator. A true pterygium is a condition found chiefly in the sunny, hot, dusty regions in the world and in people more exposed to these climatic conditions, such as fishermen, farmers, construction workers, roofers, beachgoers, and Inuit. The
Inuit are probably exposed to ultraviolet (UV) light reflected from snow.
Inuit are probably exposed to ultraviolet (UV) light reflected from snow.
Age
Pterygium is most common in the elderly, but the appearance of new cases per annum is higher in the younger age group. Pterygium is uncommon in individuals younger than 20 years of age and in people wearing glasses (14). The incidence rises suddenly in the age groups between 20 and 40 years. It has been reported in three relatives in a family in whom the onset occurred when the patients were at 4, 6, and 20 years of age (15).
Interestingly, this difference in incidence and prevalence rates related to age, geography, environmental exposure, or all, does not exist in patients with pinguecula (discussed later). Both the incidence and prevalence of pinguecula increase with age.
Sex
In general, pterygium is twice as common in male as in female patients, except in Aruba, where it is equally common in both sexes.
Heredity
Pterygium has a dominant inheritance with low penetrance. It is not the actual lesion that is transmitted, but rather the tendency of the eye to react in this special way to environmental factors. It is a commonly seen condition among the Hispanic population in the northern United States that left the geographic confines of Mexico and the sunbelt states of the United States many generations ago.
Involvement of the Second Eye
Pterygium is mostly a bilateral condition (Fig. 60-2). Like many other conditions, one eye may follow the other by months to years. The second eye, almost always, has a pinguecula that evolves into a pterygium. Most commonly, the nasal pterygia are seen in both eyes, but cases have been recorded in which one eye had a nasal and the second one had a temporal pterygium, double pterygia (Fig. 60-3), or other combinations.
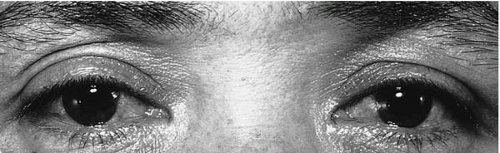 FIGURE 60-2. Bilateral primary nasal pterygia (in both eyes), and a temporal pterygium in the right eye. |
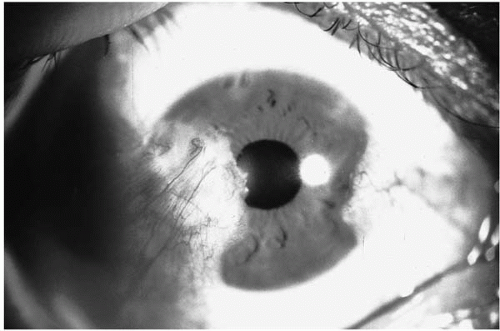 FIGURE 60-3. Double (nasal and temporal) pterygia in an eye; the temporal pterygium is growing into the papillary area, causing visual symptoms. |
ETIOLOGY AND PATHOGENESIS
The etiology of pterygium is still unknown. Its incidence related to definite geographic areas compels one to assume that certain environmental factors or agents must contribute to its development. Heat, dry climate, high winds, and abundance of dust in these geographic areas led many authors incriminate these factors as etiologic. But these fail to explain the common occurrence of pterygium in the Caribbean islands, with humid conditions year round. Desiccation from climatic conditions and a decrease of basic lacrimal secretions, with genetic predisposition, have been postulated as potent etiologic factors.
An association with exposure to UV type B (UVB) light in solar radiation has been found to be the most significant environmental factor contributing to pterygium development (14,16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28). Factors like a dry, dusty climate and genetic predisposition probably contribute to the development of pterygium. The geographic distribution of pterygium can be easily explained by the exposure to UV rays of the sun in the dry, dusty climates of deserts, in the humid conditions of the Caribbean, in Inuit from sun snow-glare, and in fishermen and beachgoers. In an investigation of more than 100,000 Australian Aborigines, researchers found a significant positive correlation between climatic UV radiation and pterygium prevalence (20). Pterygium was also significantly associated with UV radiation among fishermen on Chesapeake Bay (26,27). Similarly, the infrared spectrum of sunlight has also been blamed (28). Involuntary partial closure of the interpalpebral fissure, mostly confined to the temporal side, to avoid glare from bright sun, might explain the predominance of pterygia on the nasal side.
In a risk analysis study recently conducted in Australia, Mackenzie et al. (25) showed a several hundred-fold higher risk for development of pterygium in subjects who worked mainly on sand, and almost a 20-fold higher risk in subjects who worked in an environment that was mainly concrete,
compared with those who worked indoors. According to this study, those subjects who spent their first 5 years of life at latitudes less than 30 degrees had almost 40 times the risk of pterygium growth than those living at latitudes greater than 40 degrees, and had a 20-fold increased risk for development of pterygium if they had spent most of their time outdoors during these earliest years of life. They also found that wearing regular spectacle eyeglasses and, more important, dark sunglasses, or even wearing hats to protect eyes from exposure to sunlight had a very strong protective effect against pterygium growth (25).
compared with those who worked indoors. According to this study, those subjects who spent their first 5 years of life at latitudes less than 30 degrees had almost 40 times the risk of pterygium growth than those living at latitudes greater than 40 degrees, and had a 20-fold increased risk for development of pterygium if they had spent most of their time outdoors during these earliest years of life. They also found that wearing regular spectacle eyeglasses and, more important, dark sunglasses, or even wearing hats to protect eyes from exposure to sunlight had a very strong protective effect against pterygium growth (25).
Pinguecula
A pinguecula is a yellowish triangular patch formed by elastotic degeneration of the connective tissue, situated in the bulbar conjunctiva on either side of the cornea. It is the combined expression of changes due to age and exposure to UV light. It affects first the nasal and then the temporal side. A pinguecula appears as a roughened, raised yellowish area in the bulbar conjunctiva in the palpebral aperture near the limbus. Gradually it develops into a triangular patch with its base abutting against the cornea. Most commonly it grows to a moderate size and then ceases growing. Occasionally, nasal and temporal pingueculae may grow along the inferior limbus to meet below the cornea.
Pinguecula as a Precursor of Pterygium
Zehender, in 1869, introduced the idea that pinguecula was the precursor of pterygium (29). This hypothesis was reaffirmed by Fuchs, Parsons, and Alt, who proposed that proliferation of hyaline and elastic tissue in the connective tissue of the conjunctiva along with degenerative changes in its bulk progressed to invade the cornea and developed into a pterygium. Once pterygium has grown to a certain extent, it is impossible to locate the position of the supposed precursor or pinguecula, although it is supposed to be in the head of pterygium. This has not been confirmed histologically. This hypothesis may be acceptable for primary pterygium; however, it is known that pinguecula has no relationship to growth of recurrent pterygium.
Sugar (30) proposed that degenerative changes in pingueculae incite hyperplasia and hypertrophy of the elastic tissue and deposition of hyaline material that elevates the epithelium away from Bowman’s layer. This process causes changes at the limbus and adjoining cornea and leads to the laying down of connective tissue that contracts and pulls this fascial layer onto the cornea. D’Ombrain (31) was of the opinion that pinguecula and pterygium both are degenerative processes. If the pinguecula grew close to the limbus it would grow onto the cornea to form a pterygium; if it stayed away from the limbus, it would continue to stay as pinguecula.
Overall, it is accepted that pinguecula and primary pterygium are somehow related to each other (similar degenerative changes in response to similar environmental factors). However, recurrent pterygium is not preceded by pinguecula.
Numerous other theories have been proposed and refuted for the pathogenesis of pterygium. These include choline deficiency (32), inflammation (6,33, 34, 35, 36), allergic basis (34), degeneration (30,37, 38, 39), tissue angiogenesis factor (40), elastic tissue changes (41,42), and immune mechanisms (43). Theories to explain the development of pterygium on neoplastic, inflammatory, episcleritis, chlamydial, and allergic bases have not been well accepted. Both direct and reflected UVB radiation has been implicated in the causation of pterygium (14,16, 17, 18, 19, 20, 21, 22, 23). Mackenzie et al. (25), in a risk analysis study conducted in Australia, has suggested that the exposure of formative ocular tissue to UV radiation in the first 5 years of life probably either sensitizes or initiates a genetic, biochemical, or morphologic change that is reflected in later years of life by the development of a pterygium. This early exposure to UV light might initiate a tissue change, probably at the “putative” stem cells at the corneal limbus (25), that requires the later promoting effect of cumulative UV radiation to the ocular surface.
It is believed that UV radiation denatures corneal proteins and induces an antigen-antibody reaction that triggers fibrovascular proliferation (34). Some unidentified etiologic factor initiates a row of fibroblasts to advance into limbal cornea and penetrate the tissue in its superficial layers between Bowman’s layer and the basement membrane of the overlying corneal epithelium. Accumulation of these fibroblasts is thought to prepare a path for the head of the pterygium to enter the cornea, and on their way, the fibroblasts push Bowman’s membrane posteriorly. Gradually, Bowman’s membrane gets fragmented and the pterygium tissue grows through these fragmented areas into underlying stroma and becomes firmly adherent to the corneal tissue.
It remains unclear at this time if the invasion of cornea by pterygium tissue is initiated/triggered by degenerative changes in the basal cell layer or induced by solar radiation, by an immunologic response to altered basement membrane material, or by an inflammatory process with possible involvement of a type 1 hypersensitivity response to antigenic pollens and dust particles (40,43).
Barraquer (44) proposed a hypothesis that limbal elevation by a pinguecula, causing tear film disruption, desiccation of corneal tissue, and microulceration of adjoining corneal epithelium, was the etiopathologic factor that induced conjunctival fibrovascular proliferation to invade cornea. Dellen formation or microulceration of the corneal epithelium has been documented, but neither is a consistent finding in an active pterygium. This pathogenetic theory has lost ground because, contrary to this hypothesis, others have suggested that there is an accumulating iron line from the pooling of tears at the apex of the head of pterygium.
Recently, it has been proposed that pterygium is a growth disorder in which mutation of the p53 tumor suppressor
gene plays a vital role (45,46). Dushku and Reid (45) and Tan et al. (46) have demonstrated high p53 protein expression in the epithelium overlying the pterygium and have speculated on the existence of a p53 gene mutation in pterygia. The hypothesis that pterygium is a benign neoplastic lesion has been further supported by the finding of microsatellite instability and loss of heterozygosity in human pterygia, two common findings in tumorous tissues (47). This theory has not been well received because Onur et al. (48) found only 3 of 38 pterygia and Chowers et al. (49) found only half of the primary and recurrent pterygia had p53 immunoreactivity in their studies. Also, p53 gene mutation has not yet been demonstrated in pterygium. To refute further the theory that pterygium is a tumorous growth, Karukonda et al. (50) found proliferative activity to be similar among primary and recurrent pterygium and normal conjunctiva by using flow cytometry; another common finding in tumorous tissues. Chowers et al. (49) did not find a difference in p53 immunoreactivity between eyes with primary pterygium that did not recur and primary pterygium that was followed by recurrence of pterygium. In addition, proliferative activity of primary pterygia that recurred was similar to that of primary pterygia without recurrence, indicating that proliferative activity was not a reliable marker for recurrence (49). The results of an immunohistochemical study of human pterygium suggest that an immunopathogenetic mechanism is responsible for the pathogenesis of pterygium. It is postulated that this mechanism is perhaps triggered by preexisting conjunctivitis or microtrauma in combination with the patient’s predisposition (51).
gene plays a vital role (45,46). Dushku and Reid (45) and Tan et al. (46) have demonstrated high p53 protein expression in the epithelium overlying the pterygium and have speculated on the existence of a p53 gene mutation in pterygia. The hypothesis that pterygium is a benign neoplastic lesion has been further supported by the finding of microsatellite instability and loss of heterozygosity in human pterygia, two common findings in tumorous tissues (47). This theory has not been well received because Onur et al. (48) found only 3 of 38 pterygia and Chowers et al. (49) found only half of the primary and recurrent pterygia had p53 immunoreactivity in their studies. Also, p53 gene mutation has not yet been demonstrated in pterygium. To refute further the theory that pterygium is a tumorous growth, Karukonda et al. (50) found proliferative activity to be similar among primary and recurrent pterygium and normal conjunctiva by using flow cytometry; another common finding in tumorous tissues. Chowers et al. (49) did not find a difference in p53 immunoreactivity between eyes with primary pterygium that did not recur and primary pterygium that was followed by recurrence of pterygium. In addition, proliferative activity of primary pterygia that recurred was similar to that of primary pterygia without recurrence, indicating that proliferative activity was not a reliable marker for recurrence (49). The results of an immunohistochemical study of human pterygium suggest that an immunopathogenetic mechanism is responsible for the pathogenesis of pterygium. It is postulated that this mechanism is perhaps triggered by preexisting conjunctivitis or microtrauma in combination with the patient’s predisposition (51).
PATHOLOGY AND HISTOPATHOLOGY
Histopathologically, pterygium is a fibrovascular proliferation of conjunctival tissue onto clear cornea. Anatomically, pterygium is divided into a head, neck, and body. The head is the part on the cornea, the neck is at the limbus, and the body of the pterygium is on the sclera. An epithelial layer that histologically resembles atrophic conjunctival epithelium covers all these layers. It extends beyond its confines onto cornea. It covers the mass of pterygium that is formed by the thickened, hypertrophied, and degenerative connective tissue. Redslob (52) and Austin et al. (41) have suggested that the subepithelial tissue is fibroblastic dysplasia. Histologically it is hyperplasia, and not dysplasia. The abnormal collagen tissue is aggregated into a coiled and fibrillated pattern, similar to elastic tissue. This denatured collagen shows basophilia and can be stained with elastic tissue stains. Unlike elastic tissue, it is not digested by elastase (53) and therefore is called elastotic degeneration. Congested new blood vessels that are dispersed between hypertrophied collagen fibers richly supply this degenerative tissue.
The body of the pterygium incorporates the underlying Tenon’s capsule but spares the episcleral tissue; therefore, it is not adherent to sclera and can be easily mobilized. But, at the limbus, the absence of Tenon’s capsule makes the neck of the pterygium adherent to underlying episclera and sclera. The head of the pterygium grows in a plane between Bowman’s layer and the basement membrane of the overlying corneal epithelium. A row of fibroblasts advances in front of the apex of the head of the pterygium at this plane and “prepares” a path for the head of the pterygium to invade the cornea. In this process, Bowman’s layer is pushed posteriorly and eventually fragments and makes openings for the fibrovascular tissue of the pterygium to grow into the underlying superficial stroma of cornea. That makes the head of the pterygium firmly adherent to cornea.
In the body of the pterygium are also some tubular glands and larger spaces lined with epithelium. Both of these may result in the formation of cysts in the body of the pterygium. Histologic examination of excised pterygia also reveals a lymphocytic infiltration consisting predominantly of T cells (54).
Ultrastructural studies have revealed that both pinguecula and pterygia are composed of degenerative, basophilic, subepithelial tissue with fibers that enhance with elastic stains. Hogan and Alvarado (38) found that some fibers were sensitive to elastase, whereas others were not, concluding that the resistant fibers arose from degeneration of collagen. Austin et al. (41) found that the elastin was immature and abnormal, perhaps explaining its partial insensitivity to elastase.
The apex of the pterygium causes pooling of tears at the leading edge of slow-growing or stationary pterygia, and iron deposits settle in the form of a line central to the apex of pterygium, called Stocker’s line (55). It usually implies chronicity because rapidly growing pterygium does not allow pooling of tears in one area for periods sufficient for iron to deposit. Stocker’s line is usually not seen in active and fast-growing pterygia.
Histopathologically, primary and recurrent pterygia are two distinct entities. Recurrent pterygium is composed only of fibrovascular tissue in the absence of elastotic degeneration. It involves underlying episclera, sclera, rectus muscle sheath, and corneal stroma, and is firmly adherent to the underlying structures throughout its extent. It is highly vascularized tissue.
CLINICAL CHARACTERISTICS
Primary Pterygium
A pterygium appears as a triangular, fleshy growth almost invariably found on the nasal side slightly below the horizontal meridian (Fig. 60-1). Usually both eyes are affected on the nasal side, although unequally. Almost always it starts over the area of a preexisting pinguecula. The first
change is the appearance of gray, circumscribed opacities in the cornea near the limbus. The conjunctiva opposite these opacities shows shrinkage that is apparent by its tenseness and a displacement of the semilunar fold. As the conjunctiva encroaches on the cornea, it is preceded by the appearance of the same gray infiltrates in this tissue, at first as small islands, which gradually fuse. When fully developed, the head of the pterygium looks triangular with a blunt apex. Central to the apex are the small irregular opacities that can be seen with the slit lamp at the level of Bowman’s layer. More central to these changes, Stocker’s line may be seen, a pigmented line at the level of this membrane containing iron deposits (55). Toward the limbus, the conjunctival fold runs backward to the sclera in a tightly drawn triangular wing. At the limbal area it is referred to as the neck of the pterygium, and the fleshy mass spreading out into a fan shape on sclera is the body of the pterygium. The upper and lower borders of the body are folded; a probe can be slipped under the folds for a very short distance, and not through the full thickness because the area of adhesion is always smaller than its total breadth. These folds merge imperceptibly into the bulbar conjunctiva at the base of the pterygium and usually have considerable tension, which is manifested by the straight course of the vessels, the numerous folds, and the gross displacement of the plica semilunaris.
change is the appearance of gray, circumscribed opacities in the cornea near the limbus. The conjunctiva opposite these opacities shows shrinkage that is apparent by its tenseness and a displacement of the semilunar fold. As the conjunctiva encroaches on the cornea, it is preceded by the appearance of the same gray infiltrates in this tissue, at first as small islands, which gradually fuse. When fully developed, the head of the pterygium looks triangular with a blunt apex. Central to the apex are the small irregular opacities that can be seen with the slit lamp at the level of Bowman’s layer. More central to these changes, Stocker’s line may be seen, a pigmented line at the level of this membrane containing iron deposits (55). Toward the limbus, the conjunctival fold runs backward to the sclera in a tightly drawn triangular wing. At the limbal area it is referred to as the neck of the pterygium, and the fleshy mass spreading out into a fan shape on sclera is the body of the pterygium. The upper and lower borders of the body are folded; a probe can be slipped under the folds for a very short distance, and not through the full thickness because the area of adhesion is always smaller than its total breadth. These folds merge imperceptibly into the bulbar conjunctiva at the base of the pterygium and usually have considerable tension, which is manifested by the straight course of the vessels, the numerous folds, and the gross displacement of the plica semilunaris.
CLASSIFICATION AND STAGING OF PTERYGIUM
Progressive pterygium: An actively growing, fleshy, vascular, and inflamed-looking pterygium is called progressive pterygium. This fleshy and vascular pterygium has also been called pterygium crassum, vasculosum, or carnosum (4,6). Progressive pterygium has a very fleshy, succulent appearance and usually does not have Stocker’s line ahead of it.
Stationary pterygium: At some stage the pterygium may still look vascular, but the head of the pterygium looks pale and sparsely vascularized and stops growing and is called stationary pterygium. Stationary pterygium loses its vascular appearance and develops a Stocker’s line because of tears pooling at its apex and depositing iron into Bowman’s membrane.
Regressive pterygium: A pale, thin, papery, gray, anemic, and membranous pterygium appears to be regressing, but in reality the pterygium never gets smaller or disappears. Regressive pterygium has a gray apex resembling a corneal opacity. It is usually seen in the elderly and may represent age-related degenerative changes, as seen in other parts of the body.
Gerundo classified these three stages as: (a) proliferative papillomatous, (b) fibromatous, and (c) atrophic-sclerotic, respectively (56). Recently, Townsend (57) has classified pterygium into five groups depending on their risk of recurrence: (a) actively growing, (b) fleshy, (c) slowly growing, (d) stationary, and (e) atrophic pterygia.
Temporal
The next most common is the pterygium growing from the temporal side onto the clear cornea, representing approximately 20% of total pterygia (Fig. 60-3).
Double
Nasal and temporal pterygia presenting in the same eye are called double pterygia (Fig. 60-3) and represent approximately 20% of total pterygia.
Bilateral
Recurrent
Regrowth of the pterygium after primary excision is called recurrent pterygium. Pathologically, recurrent pterygium differs from primary pterygium; it is fibrovascular tissue growing onto the cornea without elastotic degeneration. It involves the underlying sclera, episclera, and Tenon’s capsule and grows onto corneal stroma, where it is very firmly adherent to the underlying tissues (Fig. 60-4). Recurrent
pterygium can cause restriction of ocular motility because of scar tissue or involvement of the horizontal rectus muscle sheaths.
pterygium can cause restriction of ocular motility because of scar tissue or involvement of the horizontal rectus muscle sheaths.
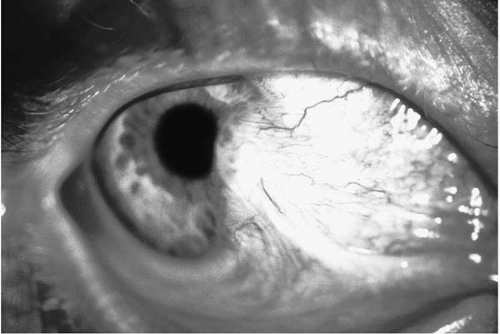 FIGURE 60-4. Recurrent nasal pterygium adherent to the underlying episclera/sclera and cornea can restrict ocular motility. |
Pseudopterygium
A pseudopterygium is the result of an inflammatory process wherein a fold of inflamed conjunctiva becomes adherent to denuded cornea near the limbus or more centrally. Marginal corneal ulceration, traumatic epithelial defects, or peripheral corneal degenerations can involve the chemotic conjunctival fold in the healing process, dragging conjunctiva across the cornea. Pseudopterygium does not respect the interpalpebral location and can be seen at any meridian on the eye. It makes a bridge of tissue growing from conjunctiva onto the corneal denuded area over limbus; a probe can be passed under its full breadth (6). It is usually unilateral and does not tend to regrow after primary breaking of the adhesions.
SYMPTOMS
Both pingueculae and small pterygia are asymptomatic. A small pterygium gives rise to no symptoms; its only disadvantage is a cosmetic blemish. A pinguecula or a pterygium may become inflamed, causing episodic inflammation, pain, and tenderness. Inflammation of pinguecula is called pingueculitis, and may resemble episcleritis. It is very rare to see inflammation of the pterygium itself.
A pterygium of significant size induces flattening of the corneal curvature in its horizontal meridian, producing with-the-rule astigmatism of up to 1.5 D. When it grows large enough to encroach on the papillary aperture, however, it obstructs peripheral vision first and eventually central vision as well. A large pterygium may cause binocular diplopia by limiting eye movements away from the pterygium body because of traction on the conjunctiva. Binocular diplopia is more common with recurrent pterygium because of its adherence to underlying sclera and episclera and sometimes because of involvement of the rectus muscle itself.
Pterygium has commonly been blamed for eye irritation, foreign-body sensation, dryness, photophobia, epiphora, and pruritus. Pinguecula has also been associated with these symptoms. These symptoms in reality are caused by the underlying dry-eye condition. UV exposure, dry climate, genetic predisposition, or any similar factor singly or in combination can cause dry-eye syndrome before the appearance of a pinguecula or pterygium. Some surgeons have recommended not operating on a pterygium in eyes with associated dryness. These symptoms start before the growth of a pinguecula or pterygium, and inadequately treated dry eye itself is believed to induce the growth of pingueculae and pterygia. These symptoms can be treated successfully with treatment of dry eye in the presence of a pinguecula or pterygium.
DIFFERENTIAL DIAGNOSIS
Pinguecula and “early” pterygium may mistakenly appear clinically similar. We emphasize that either it is a pinguecula or a pterygium. The growth on the sclera is a pinguecula; when it grows to involve cornea, it is pterygium. Clinically these are two distinct entities.
TREATMENT
Prophylaxis
Because the etiology and pathogenesis of pterygium growth are unclear, the role of prophylaxis is also uncertain. Theoretically, preventing or limiting exposure to UV light might be of some help. A change of environment might not be feasible or practical. Protection of the eyes by regular spectacles, dark sunglasses, or hats when exposed to the sun or irritating environmental conditions could certainly do some good, as suggested by Cameron (14), Rosenthal et al. (58,59), and Mackenzie et al. (25). Cameron (14) found in Australia that the rate of incidence of pterygium was reduced from an average of 15% to 3% among those who had worn glasses constantly from before the age of 15 years. Mackenzie et al. (25) found that the normal population that did not wear regular spectacles was at a threefold higher risk for development of pterygium compared with the population that wore regular spectacles. The population that wore dark sunglasses when exposed to the sun was five-fold better protected than the general population against pterygium growth. This association has also been found with wearing a hat in the sun. Mackenzie et al. (25) has recommended avoidance of exposure to UV light, especially in the first 5 years of life.
Medical Treatment
Surgical Treatment
The only effective treatment for pterygium is surgery. However, none of the surgical procedures is perfect and
universally accepted because of high recurrence rates. Since the time of Susruta, mankind has tried almost every imaginable procedure to remove pterygia with the hope that there would be no recurrence. Even in ancient times the problems of pterygium management were recognized. Susruta wrote, “Any remnant of the pterygium should be removed with a scarifying ointment to prevent recurrence” (3). According to Rich et al. (60), “to manage pterygia, we can incise, excise, bury, transplant, graft, freeze, burn, cauterize, diathermize, divulse, evulse, chemically assault, irradiate or simply leave them to fate.” The many therapeutic options available to manage pterygia imply that no single one is completely effective. Almost all (91.6%) recurrences appear by 360 days after surgery. It has been suggested that 1 year is the optimal follow-up time to identify recurrence of pterygium (61).
universally accepted because of high recurrence rates. Since the time of Susruta, mankind has tried almost every imaginable procedure to remove pterygia with the hope that there would be no recurrence. Even in ancient times the problems of pterygium management were recognized. Susruta wrote, “Any remnant of the pterygium should be removed with a scarifying ointment to prevent recurrence” (3). According to Rich et al. (60), “to manage pterygia, we can incise, excise, bury, transplant, graft, freeze, burn, cauterize, diathermize, divulse, evulse, chemically assault, irradiate or simply leave them to fate.” The many therapeutic options available to manage pterygia imply that no single one is completely effective. Almost all (91.6%) recurrences appear by 360 days after surgery. It has been suggested that 1 year is the optimal follow-up time to identify recurrence of pterygium (61).
Indications for Surgery
The primary indication for pterygium excision is decreased visual acuity because of encroachment of the pterygium into the visual axis or the irregular astigmatism induced by the growth. Surgery may also be indicated because of the breakup of the precorneal tear film. Other reasons for surgical intervention include ocular irritation and discomfort unresponsive to lubrication, restricted ocular motility, binocular diplopia (mostly due to recurrent pterygium), or the progression of the pterygium toward the visual axis. Surgery may also be indicated in cases where the pterygium, or even pinguecula, restricts wearing of contact lenses. Difficulty in performing corneal refractive surgery has also been added to the list of surgical indications for pterygium excision. Most patients seek surgical excision of the pterygium for cosmetic reasons, but they need to be informed of the high recurrence rate and the scarring left after pterygium excision.
Current Surgical Procedures for Pterygium Treatment
Bare-Sclera Excision
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


