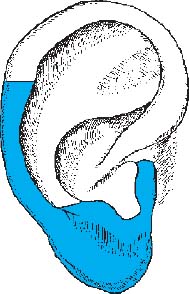
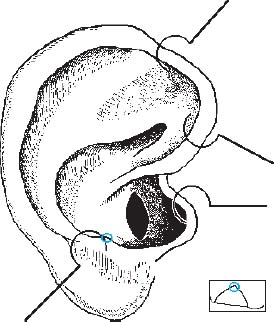
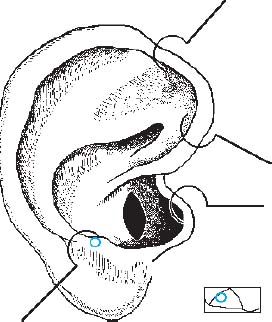
Because of the vagueness of the ear map in effect at that time, Bahr asked me in 1994 to check the accuracy of the localizations of the central nervous system, the cranial nerves, and the autonomic nervous system (VAS-controlled testing by means of resonance to the respective anatomical material, using Wala test ampoules). This reevaluation resulted in new localizations on the ear for some structures of the nervous system (e.g., the hypothalamus, some cranial nerves, the nuclei of origin, and some ganglia of the autonomic nervous system). Location: • The central nervous system projects essentially onto the descending helix and the ear lobe (localization of the ectoderm, see Germ Layers, p. 8). • Here, too, the general rule applies: the sensory portion of the reflex zone is located on the front of the ear and the motor portion on the back of the ear. The projection of the head of the inverted embryo fills the entire lobule (Nogier). Accordingly, the main portions of the brain and the head (sensory organs, temporomandibular joint, teeth, maxillary sinuses, facial muscles) are represented on the ear lobe (see Germ Layers, p. 8, and Head, p. 99). The brain projects onto the entire ear lobe. The bony skull projects only onto the antitragus; the area is not identical with the projection of the brain. The projected embryo lies with its back against the posterior edge of the ear (descending helix). Accordingly, the reflex zone of the spinal cord is in this area (sensory portion on the front of the ear, motor portion on the back of the ear). Certain parts of the central nervous system are not represented on the descending helix and lobule, namely, the commissural fibers, the thalamus, and the hypothalamus. Their exact localizations will be described in the respective sections. Note: Because many of the reflex zones will not come to mind easily in the daily clinical routine or practice, possible indications are also provided in this chapter. Fig. 5.1 Central nervous system As a refresher and for a better understanding of the following description of auriculomedical details: The precentral area is especially important in all neurological disorders that affect motor functions in one way or another (this area is often neglected in auriculotherapy). Of equal importance is the postcentral area on the most anterior gyrus of the parietal lobe, because it is the terminal site of all sensory fibers. Location: • The four large lobes of the telencephalon (frontal, temporal, parietal, and occipital lobes) project onto the anterior and middle ear lobe and, in part, onto the outer surface of the antitragus. Indications: • See discussion of the individual cerebral lobes. Fig. 5.2 Fig. 5.3 Location: • This is the area in the most anterior part of the ear lobe, below the intertragic notch and reaching down to the Main Omega Point. • The precentral gyrus projects on the back of the ear near the attachment of the ear lobe. • Broca’s motor speech area projects on the back of the ear near the Precentral Gyrus Zone (search for the active point). Indications: • In case of hemorrhage in, or injury to, the frontal lobe it makes sense to try supportive therapy by ear acupuncture (especially when the motor speech area is affected). • Combination of ear acupuncture with laser acupuncture on the skull (in the corresponding region) may be favorable. • An affected area of the precentral gyrus can be directly influenced, for example, in infantile cerebral palsy and the like (use the reflex zone on the back of the ear). Note: The frontal lobe includes: • the precentral area (precentral gyrus), hierarchically the highest motor center where the pattern of movement is designed and transmitted to deeper-lying centers (basal ganglia, cerebellum, etc., where the somatotopic arrangement results in an inverted homunculus); • the frontal eye field, through which conjugated eye movements are controlled independently of the eye-muscle nuclei; • Broca’s motor speech area in the inferior frontal gyrus of the dominant hemisphere. Damage (injury, hemorrhage) causes motor aphasia, i.e., the patient is no longer able to form words or to speak, although the speech muscles are not paralyzed and speech comprehension is intact. Fig. 5.4 Location: • On the ear lobe, lateral to the Frontal Lobe Zone. • The postcentral gyrus projects onto the boundary between these two zones. Indications: • For example, as supportive therapy in case of injury to this region. Note: The postcentral gyrus is the most anterior gyrus of the parietal lobe where all sensory fibers terminate (somatosensory cortex). Impairment in the region of the parietal lobe may result in various forms of agnosia. While sensations are still perceived, objects are no longer recognized as what they are. Fig. 5.5 Location: • On the ear lobe and lower edge of the antitragus, lateral to the Parietal Lobe Zone. Of particular importance for the practical approach: • The auditory area of the temporal lobe projects as Auditory Line on the ear lobe. Indications: • As supportive therapy in case of injury to this region, especially when Wernicke’s speech area is affected. • Special forms of tinnitus. Note: Wernicke’s speech area is located in the posterior region of the superior temporal gyrus of the dominant hemisphere. Injury causes deficit in word comprehension (sensory aphasia): words are used in senseless combinations (word salad, empty speech), language comprehension is impaired. Injury to the angular gyrus causes word blindness, i.e., inability to read (alexia) and to write (agraphia). The acoustic radiation (with origin in the lateral geniculate body) terminates in the transverse temporal gyrus, deep below the operculum. Location: • A horizontal line on the antitragus (Nogier described this line before he even knew the exact projection of the cerebral lobes). • The line needs to be pierced with several needles on the ear of the affected side, in most cases with silver needles (it is essential to decide on the needle metal by using the point finder). Application: • Tinnitus, Ménière’s disease, sudden deafness. Fig. 5.6 Temporal lobe Fig. 5.7 Auditory Line Location: • On the outer surface of the antitragus, also on the back of the ear in the corresponding area. Indications: • As accompanying therapy in hemianopia, for example, in case of infarction of the occipital lobe. The optic radiation terminates here in the calcarine sulcus. Location: • The corpus callosum projects onto the entire tragus. Indications: • Especially important in all disorders associated with problems of laterality (e.g., bed-wetting, childhood asthma, learning difficulties, suppressed left-handedness). • Laterality problems may result from disease, but may also cause disease. Note: Physiologically, the corpus callosum plays an important role in balancing the two cerebral hemispheres. It is related to laterality and laterality disorders because it is the most important and largest commissure of the cortex: The commissural fibers crossing through the corpus callosum connect the cortices of both hemispheres (left-right connections). These connections involve similar as well as different regions of the two hemispheres. Fig. 5.8 Occipital lobe Fig. 5.9 Corpus callosum Location: • On the inside of the antitragus where the inferior concha merges with the ascending wall of the antitragus. • When pulling the antitragus outside, a depression becomes visible on its inner wall. The Thalamus Point is located at its deepest point. Indications: • In all severe conditions of pain, possibly as a supplementary point. • Corresponds to Point LI-4 of body acupuncture. Note: The thalamus (Greek: thalamos, inner chamber) may be regarded as gateway and distribution station for all afferent systems to the phylogenetically younger telencephalon structures which permit targeted and conscious behavior. It is therefore also known as the “gate to consciousness.” It plays a key role in processing and modulating pain. Fig. 5.10 Thalamus Location: • Superior and lateral to the Thalamus Point, in the wall ascending from the inferior concha to the antitragus. Indications: Still a neglected reflex area in auriculotherapy, it should be tested in the following conditions (the needle metal needs to be decided): • arterial hypertension and hypotension, • insomnia, • overweight and eating disorders, • fertility disorders and other hormonal problems, • sexual problems, • excessive perspiration, • autonomic imbalance and everything associated with it. Note: The hypothalamus contains the higher control centers of the autonomic nervous system which coordinate the essential regulatory processes of the body: • thermoregulation, • sleeping-waking rhythm, • regulation of blood pressure, • regulation of respiration, • food intake (feeding center and satiety center), • fat metabolism, • fluid balance (water and electrolytes), • sexual function, • perspiration. The hypothalamus is the center of all the essential homeostatic processes of the body. Fig. 5.11 Hypothalamus Location: • The adenohypophysis (anterior pituitary gland) projects onto a relatively large area in and around the intertragic notch. Commonly used points, such as Prolactin Point, ACTH Point, TSH Point, Gonadotropin Point, are also found here. • The neurohypophysis (posterior pituitary gland) projects lateral to the anterior part of the antitragus. Indications: • Analogous to the action of the individual hormones; for example, therapy when children are desired, hypermenorrhea, difficult menstruation, mastopathy, stimulation of lactation (Prolactin Point) or milk ejection (Oxytocin Point). • The choice of needle metal is specified by the initial clinical situation and depends on the need for stimulation or sedation (use gold or silver needle, respectively). • In any case, the point will need to be tested for its potential, as usual, by using the 3-volt-hammer or point finder. Note: • Anterior lobe of pituitary gland (adenohypophysis): production of FSH, LH, TSH, ACTH, GH (STH), prolactin. With the exception of the two latter hormones, these are glandotropic hormones which control the function of other secondary endocrine organs. The secretion of hormones is controlled by the releasing hormones of the hypothalamus. • Posterior lobe of pituitary gland (neurohypophysis): The hormones oxytocin (milk ejection) and vasopressin (regulation of blood pressure), which are produced by the hypothalamus, are stored here and released when needed (hypothalamic–pituitary system). Fig. 5.12 Prolactin Point Location: • When children are desired, the right ear usually bears the Silver Point (the needle metal needs to be decided). • Just above the ACTH Point. Indications: • When children are desired (because hyperprolactinemia is often present, use silver needle on the right ear). • Supports lactation (use gold needle). • Hormonal disorders; for example, oligomenorrhea or amenorrhea associated with hyperprolactinemia (use silver needle). ACTH Point Location: • The right ear normally bears the Gold Point. • In the anterior corner of the intertragic notch where the notch ascends to the tragus. Indications: • ACTH stimulation; for example, in all cases of allergies. • For supporting amalgam elimination use gold needle on the right ear. • Corresponds to Point LR-13 of body acupuncture. TSH Point Location: • Requires stimulation or sedation depending on the syndrome. • Just behind the ACTH Point (in posterior direction toward the antitragus). Indications: • Predominantly diagnostic when latent hypothyroidism is suspected; supports the therapy in case of disease. Gonadotropin Point (FSH/LH Point) Location: • The right ear normally bears the Gold Point (this may vary with the syndrome; hence, the needle metal needs to be decided). • On the anterior outer bulge of the antitragus, about 2mm inferior to the upper reflection. When the antihelix is imagined as a snake, the antitragus forms the head of the snake, while the Gonadotropin Point forms the eye. Indications: • Mainly during menopause in combination with the Estrogen Point. Oxytocin Point Location: • On the antitragus, posterior to the Gonadotropin Point. The Vasopressin Point is also located very close to it. Indications: • Supports milk ejection during lactation. Fig. 5.13 Location: • On the outside of the antitragus, about 2mm below the upper edge (testing was done with the following substances in the ampoules: hippocampus, cingulate gyrus, amygdaloid body). Indications: • Anxiety, emotional depression associated with general autonomic hyperexcitability. The reflex area of the limbic system is certainly worthy of more attention in auriculotherapy. (After needling is complete, search this area for low-energy points.) Note: The entire limbic system is largely responsible for emotional nuances of behavior in general as well as for emotional reactions (anger, fear, affection, anxiety, etc.) and is probably also involved in cerebral functions such as memory and learning. The system includes the limbic cortex (hippocampus, parahippocampal gyrus, cingulate gyrus, amygdaloid gyrus, mamillary body, habenular nuclei), the limbic mesencephalon, and the extramural and intramural limbic fibers. It is the control center directly superior to the hypothalamus and regulates the endocrine and autonomic nervous systems (visceral brain). Fig. 5.14 Location: •
Central Nervous System—Overview
Cerebral Lobes—Overview
Cortex
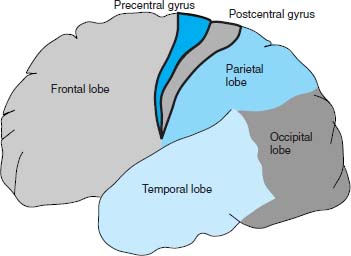
1 Frontal lobe
2 Parietal lobe
3 Temporal lobe
4 Occipital lobe
5 Precentral gyrus
6 Postcentral gyrus
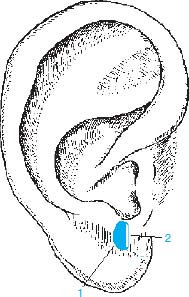
Frontal Lobe
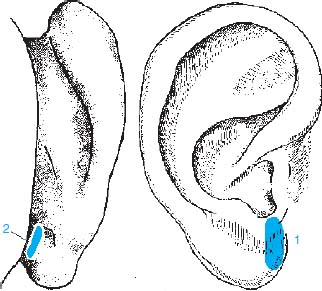
1 Frontal lobe
2 Precentral gyrus
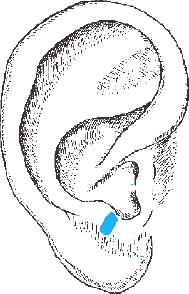
Parietal Lobe
1 Parietal lobe
2 Postcentral gyrus
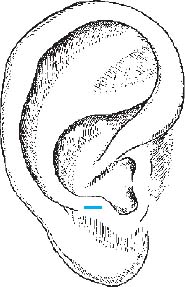
Temporal Lobe
Auditory Line
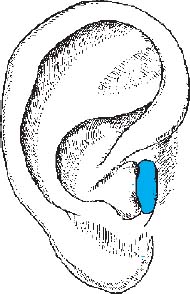
Occipital Lobe
Corpus Callosum

Thalamus
Hypothalamus
Pituitary Gland
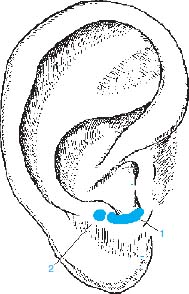
1 Adenohypophysis
2 Neurohypophysis
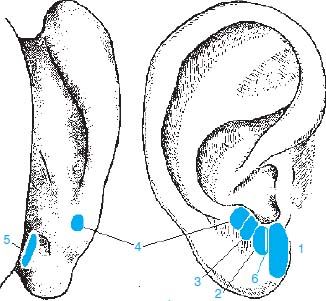
Pituitary Gland Points
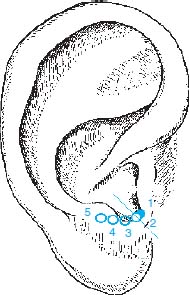
1 Prolactin Point
2 ACTH Point
3 TSH Point
4 Gonadotropin Point (FSH/LH Point)
5 Oxytocin Point
Limbic System
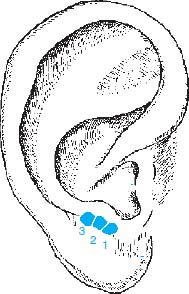
1 Cingulate gyrus
2 Amygdaloid body
3 Hippocampus
Cerebellum
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


