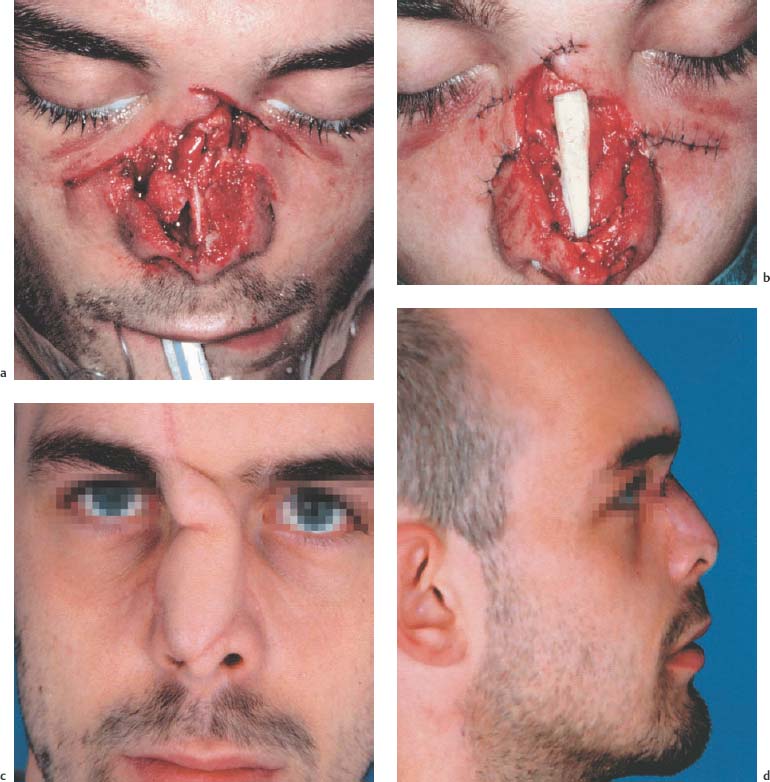
15 Principles of Wound Management 2. Sufficient administration of anesthesia must be ensured. Children and patients with more extensive trauma should be treated under general anesthesia. A local anesthetic with epinephrine must be used in the head and neck region to aid hemostasis and prolong the time anesthetic remains in the tissue. Never anesthetize from the wound edges into the surrounding tissues, but always from the surrounding tissues toward the wound edges. Use of conduction anesthesia is preferred. 3. Thorough inspection (foreign bodies, neurovascular injuries) and thorough wound cleansing (hydrogen peroxide, polyvidone iodine, brushes) prior to treatment. 4. Careful hemostasis using (monopolar or bipolar) coagulation rather than sutures that tear through and traumatize tissues. 5. Avoid wound excision. However, devitalized, necrotic tissue components must be carefully (magnifying eye loupe, operating microscope) removed. Irregular wounds are sutured by initial fixation of matching wound edges with subcutaneous sutures. This eliminates tissue tension, allowing easier closure of remaining spaces in between. 6. Use the finest, atraumatic suture material and fine instrumentation. Avoid additional trauma to the wound edges caused by grasping tissue with sharp forceps. Atraumatic forceps and fine wound hooks must be readily available. 7. Wounds are always closed from the inside out (bone, mucosa, muscle, skin). Suturing of cutaneous wounds is always done with subcutaneous sutures. Suture from free to attached edges and from thinner to thicker skin margins to allow exact coaptation of wound edges. 8. Always ensure sufficient drainage of the wound area. 9. Antibiotics should be administered as needed; tetanus vaccination status must be checked. 10. Use supportive bandaging and change dressings daily. Uncompromising removal (brush) of foreign bodies embedded in the skin is of the utmost urgency as otherwise permanent traumatic tattooing results. This is followed by cleansing and disinfection of wound surfaces. Oozing hemorrhage is treated by administration of an astringent or hemostatic. External agents with antibiotics are now obsolete. Bleeding abrasions are covered with an ointment compress or a sterile gauze compress. Wound dressings should not adhere to the wound and must ensure that the wound surface remains moist. Fixation of the dressing is with a tubular dressing or cohesive gauze padding. Elastic bandage wraps, which are applied with slight pressure, are an alternative, as the compression effect supports re-epithelization. Primary care of mild abrasions includes application of a spray dressing or a ready-made dressing and then open treatment. Attention should be paid to sufficient tetanus prophylaxis. Objects firmly positioned in the wound must always be left in place until definitive treatment, in order to avoid heavy bleeding. It may be necessary to place padding around the object. A sterile bandage should be applied until definitive treatment. Radiographs should be taken to determine the position of any radiopaque object firmly lodged in the wound. If damage to large vessels or nerve trunks is suspected, the penetrating object should only be removed with surgical standby. Following removal thorough clinical evaluation of the wound tract is necessary to determine extent and depth of the wound as well as to rule out injury to deeper organs, vessels, tendons, and nerves. The wound may be closed after being cleaned, assuming there is no suspicion of contamination. Attention must be paid to ensuring good drainage. Perioperative antibiotic treatment is required in injuries of the pharynx or paranasal sinuses. Additional administration of antibiotics depends on the type of injury, tissue damage, and type of operation. Careful documentation of position and direction of the wound tract is important if there is third party involvement. It is absolutely crucial that the penetrating object (e. g., knife) be secured. Attention should be paid to adequate tetanus prophylaxis. Bleeding must be controlled with application of a light compression bandage. Attention should be paid to good coaptation of wound edges. If needed, wound edges can be coapted with wound closure strips. The full extent of injury should be determined at the beginning of treatment. If neural injury is suspected (e. g., facial nerve), functional diagnosis is absolutely essential for identifying the extent of damage and to be able to perform primary reconstruction. Cleansing of the wound follows with hydrogen peroxide and sterile sodium chloride solution. The skin is closed using interrupted or intracutaneous continuous suturing and covered with a sterile dressing (dry protective dressing). Sutures are removed after between 5 days (lids) and 10 days (scalp). Deeper, older wounds must be explored and cleansed, followed by prudent excision of wound margins and drainage placement. For facial injuries, unlike wounds involving other body parts, primary wound closure can be attempted, even for older wounds. Attention should be paid to adequate tetanus prophylaxis. A sterile protective bandage should be applied, or, in the case of hemorrhage, a sterile compression bandage. Generous wound excision and secondary suturing must be avoided in the facial region. Necrotic areas must be removed, however (magnifying eye loupe, operating microscope), and the wound sufficiently drained. Primary coaptation of wound margins is desirable. Grafting techniques are used for defects (Fig. 15.1). Antibiotic prophylaxis is mandatory in all bite injuries. If there is potential rabies contamination, any suspicion of infection demands initiation of active immunization. Passive immunization with human rabies immunoglobulin in parallel is advisable. Tetanus prophylaxis should be administered if there is any uncertainty of patient immunity. Human bite wounds carry a risk of infection with HIV, hepatitis B, or hepatitis C. If infection is suspected, serologic status of the patient and the biter must be determined. Fig. 15.1 Bite wound to the nose with loss of skin and cartilage. a Situation at the beginning of treatment: extensive loss of skin and cartilage. b Closure of the skin defect, reconstruction of the bony/cartilaginous nasal skeleton with costal cartilage. c Healed forehead flap, which was used for reconstruction of the external nose. d View of the lateral aspect of the nose after separating the flap pedicle. A compression bandage is used to achieve hemostasis. For extensive injury in the oral cavity, immediate intubation, tracheotomy, or, in an emergency, cricothyrotomy, is necessary. Graze wound: Treatment is with mechanical cleansing of the wound to remove embedded foreign bodies. After ruling out associated injuries (e. g., nerves), primary wound closure, with grafting techniques if needed, should be attempted. Through-and-through wounds and retained missiles: In retained missile wounds, the embedded foreign bodies must be removed (image amplifier). Endoscopic techniques are useful. For through-and-through injuries, the wound should be cleaned, drained, and any defect injuries managed. If there are extensive defect wounds, definitive treatment should be after a period of several days as secondary necrosis can occur with this pattern of injury. Paintball injury: The penetration of foreign bodies into tissues requires ample, possibly repeated, wound cleansing, with the goal of complete removal of foreign material. Attention should be paid to adequate drainage of the wound area after closure. For forensic purposes, attention must be paid to careful documentation of the missile tract and any gunpowder burns (photos) for all missile wounds. Any projectiles must be secured. Attention must be paid to adequate infection and tetanus prophylaxis.
The Ten Commandments of Wound Management
 1. Thorough patient history, possibly including photographic documentation.
1. Thorough patient history, possibly including photographic documentation.
Abrasions
Immediate Management/Treatment
Puncture Wounds
Immediate Management
Treatment
Cut Wounds
Immediate Management
Treatment
 Small, superficial wounds can be coapted with wound closure strips.
Small, superficial wounds can be coapted with wound closure strips.
 Superficial, clean, wounds with smooth margins are treated with layered wound closure and, if needed, drained for 24 hours.
Superficial, clean, wounds with smooth margins are treated with layered wound closure and, if needed, drained for 24 hours.
Bite Wounds
Immediate Management
Treatment
Missile Wounds
Immediate Management
Treatment
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


