Study
Monocular blindness (%)
Bilateral blindness (%)
Primarily Caucasian Study [30]
27
9
Temba Glaucoma Study [31]
58
Chen Study [32]
14.6
6.4
In African-Americans, the incidence of glaucoma is up to six times higher in certain age groups compared to whites. POAG in blacks is more likely to lead to irreversible blindness. Glaucoma occurs 10 years earlier and progresses more rapidly in black compared to white patients. Historically, blacks tend to be less aware they may have glaucoma with its sight-threatening consequences, and they respond more poorly to therapy, whether medical or surgical [33].
Glaucoma patients are frequently unaware of their disease. Rarely, patients will present having actually noticed visual field changes. Indeed, glaucoma is often referred to as the “sneak thief of sight.” In most industrial societies, more than 50 % of those affected are unaware of their condition [1, 34]. The percentage of undiagnosed glaucoma may exceed this value in third world nations. Fifty-seven percent of POAG was undiagnosed in the Thessaloniki Eye Study, with a lack of regular visitation to an ophthalmologist being a major reason for the underdiagnosis [35]. In the Melbourne Visual Impairment Project, 50 % were previously undiagnosed [18]. Seventy-four percent were undiagnosed in the Blue Mountain Study [23], and 55 % lacked an awareness of their glaucoma in the Baltimore Eye Study [20]. In the aforementioned Temba Glaucoma Study, 87 % of patients were previously undiagnosed [31], while an even greater 93 % were undiagnosed in a rural South India study [36]. In the 9-year Barbados Eye Studies, over one half of the participants with POAG were unaware of their diagnosis. The lack of knowledge of their disease was four times more likely when opticians or optometrists were the regular eye care provider compared with ophthalmologists [37, 38]. Because open angle glaucoma has no early symptoms, periodic eye exams are an important component of the battle against glaucoma. These exams should become more frequent with age, perhaps every year for patients over 60 years of age. The overwhelming patient unawareness of their glaucoma is highlighted in Table 12.2.
Table 12.2
Patient lack of awareness of glaucoma
Study | Percent unaware of diagnosis |
|---|---|
Framingham Study | >50 |
Thessaloniki Eye Study [35] | 57 |
Melbourne Visual Impairment Project [18] | 50 |
Blue Mountain Study [23] | 74 |
Baltimore Eye Study [20] | 50 |
Temba Glaucoma Study [31] | 87 |
South India Study [36] | 93 |
Barbados Eye Studies [38] | >50 |
Definition
Glaucoma is an optic neuropathy with characteristic, usually progressive, visual field loss and optic nerve cupping, often associated with “elevated” intraocular pressure (IOP). As we have seen above in the population-based studies, “elevated” IOP is not necessary to make the diagnosis of primary open angle glaucoma (POAG). There are many varieties of glaucoma. Glaucoma classification systems are important in terms of treatment and prognosis. Accepted classification systems divide glaucoma into broad categories, including open versus closed angle glaucomas and primary versus secondary glaucomas. Many of these varieties of glaucoma are discussed in detail in other chapters in this book. Here we will discuss primary open angle glaucoma, or glaucoma with a visually open anterior chamber angle or “drain” (by gonioscopy) (see Figs. 12.1, 12.2, 12.3, and 12.4) and without underlying, secondary ocular disease. If the angle formed by the iris plane, the ciliary body face, and the posterior cornea is greater than 20°, it is considered open. Otherwise, angles are described as either narrow or closed. POAG is the most common of the glaucomas, accounting for up to 75 % of all glaucomas.

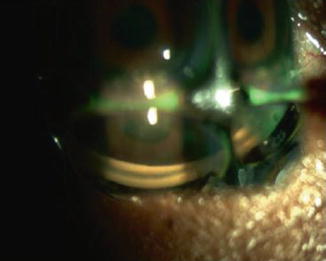


Fig. 12.1
African-American diabetic male with neovascularization of iris, ectropion uvea, and angle closure glaucoma
Fig. 12.2
Zeiss-style 4-mirror lens on the eye of the patient in Fig. 12.1. The angle is closed with no angle structures visible
Fig. 12.3
Gonio lens on the eye of a patient with an open angle and visible angle structures
Fig. 12.4
Gonio lens on the eye of a patient with narrow angles
Genetics
Von Graefe first recognized clusters of glaucoma patients within a family in 1869 [39]. Duke-Elder subsequently described an autosomal dominant form of glaucoma [40]. Over the years, several modes of inheritance have been proposed, including sex-linked recessive, autosomal recessive, autosomal dominant, and multifactorial [41]. Referencing the Finnish cohort study, Teikari, in 1987, estimated the heritability of POAG at 13 % [42]. Chang and coworkers studied the heritability of intraocular pressure and cup to disc ratio in an older population and concluded that C/D ratios are highly heritable, while IOP is moderately heritable [41]. Working with patients, their family members, and ophthalmologists, genetic researchers have identified 70 genes, loci, and alleles that either cause glaucoma or syndromes associated with glaucoma. The glaucomas occurring as a result of these genes include infantile glaucoma, juvenile glaucoma, syndromic glaucoma, and some normal pressure and high pressure glaucomas. These glaucomas are the tip of the iceberg, as they represent only a small portion of all glaucomas [43]. It is hoped that development of genomic testing panels will allow earlier detection of (1) patients at risk for glaucoma, (2) aggressive forms of glaucoma, and (3) patients responsive to a particular treatment. Armed with this knowledge, clinicians may tailor treatment of glaucoma on a personal or customized level.
Risk Factors
Risk factors are characteristics that may be causal with respect to a particular disease. They predate the development of the disease, and they may play a significant role in development of the disease. Of the many risk factors associated with open angle glaucoma, elevated intraocular pressure is the leading risk factor and the only currently modifiable one. Upwards of six million people in the USA have elevated intraocular pressure without demonstrable perimetric visual field damage [12, 44, 45]. It is important to understand that while no degree or level of IOP is diagnostic of glaucoma, glaucomatous optic disc damage may occur at almost any IOP but is more prevalent as IOP increases. Furthermore, as we will show below, lowering IOP, regardless of the level at which disc and field damage originally occurred, seems to be beneficial in slowing or halting progression of visual field loss.
Prediction of which ocular hypertensive patients are most likely to develop glaucoma could allow a reduction of the prevalence and severity of primary open angle glaucoma via the institution of earlier therapy. The Ocular Hypertension Treatment Study (OHTS) showed that reducing intraocular pressure a modest 20 % in ocular hypertensive patients lowered the 5-year incidence of glaucoma from 9.5 % in the control or untreated group to 4.4 %—a 60 % drop [46]. Treating all ocular hypertensives would subject many patients to unnecessary treatment, as well as the associated costs, side effects, and inconvenience. A more reasoned approach identifies those patients at high risk, and either initiates early treatment or pigeonholes those patients into closer monitoring. The European Glaucoma Prevention Study Group (EGPS) validated the results of the OHTS. In the OHTS observation group, the 5-year cumulative probability of developing open angle glaucoma was 9.5 %, while in the EGPS observation group, the 5-year cumulative probability was higher at 16.8 %. In the OHTS control group (no treatment), baseline older age, higher IOP, larger vertical cup/disc ratio, thinner central corneal thickness (CCT) measurement, and greater pattern standard deviation (PSD) were predictive factors for the development of primary open angle glaucoma [47]. Interestingly, in the initial OHTS analysis, self-reported diabetes was protective with respect to the future development of glaucoma [47]. Subsequent publication did not support the protective association between diabetes and POAG and suggested further study to clarify the association between diabetes and POAG [48]. The EGPS validated these same predictive factors [49]. Hazard ratios were the same among both the OHTS and the EGPS, as well as pooled data from two other studies [49–51]. Additional risk factors were uncovered during follow-up of the trials, including intraocular pressure reduction [46], intraocular pressure fluctuation [52], optic disc hemorrhages [53], and use of antihypertensive medications [54].
Mean IOP reduction, mean IOP, presence of optic disc hemorrhages, and use of systemic diuretics are all predictors for the development of open angle glaucoma. These associations have been supported by the OHTS [46], the Early Manifest Glaucoma Trial (EMGT) [55, 56], and the EGPS studies. The greater the decrease in IOP, the lower the mean IOP, and the smaller the area under the curve of IOP, the less the risk of glaucoma. In the EGPS, for each 1 mmHg higher IOP per 12-month period, the increase in risk of developing OAG is 9 % for a 5-year period [57]. Analysis of the EMGT data showed there was a 10–13 % protection for each lower 1 mmHg in intraocular pressure observed during a 5-year follow-up of POAG patients.
Controversy exists with respect to diurnal fluctuation and intervisit fluctuation of intraocular pressure as risk factors for the development and/or progression of glaucoma. The EGPS showed that intervisit IOP fluctuation over follow-up was not a risk factor for the development of glaucoma. In contrast, the Advanced Glaucoma Intervention Study (AGIS) [58] and other studies reported that intervisit fluctuation was a risk factor for progression of POAG glaucoma [59–62]. In ocular hypertensives, Bengtsson et al. showed there was no association between diurnal fluctuation repeatedly measured over a 10-year follow-up with conversion to POAG [63]. In the EMGT, he reported no association between diurnal fluctuation and progression of OAG in patients [64].
Medeiros and Weinreb have reported that long-term fluctuations do not appear to be significantly associated with the risk of developing glaucoma in untreated ocular hypertensive subjects. Their study included 252 eyes of 126 patients with ocular hypertension. Forty eyes of 31 subjects developed glaucoma. The mean IOP in converters was 25.4 mmHg, compared to 24.1 mmHg in eyes that did not convert. Intraocular pressure fluctuations were 3.16 mmHg in converters and 2.77 mmHg in non-converters [65].
According to a study by Leske and Heijl et al., treatment and follow-up IOP had a marked influence on progression, regardless of baseline IOP. Other significant factors were age, bilaterality, exfoliation, and disc hemorrhages. Optic disc hemorrhages are a well-known risk factor for development and/or progression of glaucoma [53, 56, 66–69]. Meanwhile, lower systolic perfusion pressure, lower systolic BP, and cardiovascular disease history emerged as new predictors, suggesting a vascular role in progression. Another new factor was CCT [70]. In the EGPS, the use of diuretics was associated with conversion to open angle glaucoma but the presence of systemic hypertension was not [57]. This effect may be due to a lower perfusion pressure, as low diastolic perfusion pressure has been associated with POAG [71, 72].
Treatment or over-treatment of systemic hypertension may cause a marked decrease in systemic blood pressure. This, in turn, may cause a chronic decrease of ocular blood flow and ultimately loss of retinal ganglion cells. In the Egna-Neumarkt Study [73], a positive correlation was discovered between systemic blood pressure and IOP, and an association was found between POAG and systemic hypertension. Lower diastolic perfusion pressure is associated with a marked, progressive increase in the frequency of hypertensive glaucoma. The study found no relationship between systemic diseases of vascular origin and glaucoma. Poor perfusion of tissues can occur in the context of either hypertension or hypotension. Hypertension works by increasing peripheral vascular resistance in small vessels, while hypotension works by producing insufficient perfusion pressure of the optic disc. Low diastolic blood pressure, in the below 70 mmHg range, increased the incidence of glaucoma. In a Baltimore study, this association began at diastolic perfusion pressures less than 50 mmHg [71], while 23 % of the Egna-Neumarkt glaucoma cases had ocular perfusion pressures less than 50 mmHg. It should be noted that this is not the most important mechanism of glaucoma in terms of frequency. Additionally, no link was found between glaucoma and the presence of diseases of other vascular tissues—angina, infarct, stroke, TIA, and intermittent claudication. These findings were similar to those of Armaly, Drance, and Klein and Klein [74–76]. However, the findings were in disagreement with a significant number of other authors [77–83].
In the Thessaloniki Eye Study, nonglaucomatous individuals with systemic hypertension, whose medical treatment had induced a low diastolic blood pressure, had larger cup areas and cup/disc area ratios as assessed by HRT compared to individuals with higher diastolic pressures [84]. Dielemans et al. found that systemic blood pressure and hypertension are associated with IOP and high tension glaucoma (IOP > 21 mmHg), but there is no association between blood pressure or hypertension and normal tension glaucoma [85]. The EGPS, Thessaloniki Eye Study, and the Punjabi report all confirmed that either treated hypertension is a risk factor for glaucoma progression or there is a potential association between diuretics usage and conversion to glaucoma [57, 84, 86].
Nocturnal dips in blood pressure may be a risk factor in glaucoma. Nocturnal pressure parameters, except pulse pressure, have been found to be lower in the patients with progressive field defects [87]. Graham and Drance reported that nocturnal dips in blood pressure were lower in patients with progressive field loss compared to patients with stable fields. This occurred in the context of good intraocular pressure control [88].
Piltz-Seymour et al. showed that laser Doppler flowmetry detected circulatory abnormalities in POAG suspects without manifest visual field changes. Decreases in flow in glaucoma suspects paralleled those of patients with POAG. The data suggested that compromised optic nerve blood flow occurs early in glaucoma development and does not develop solely as a result of glaucoma damage [89].
Thinner central corneal thickness (CCT) is thought by many to be a risk factor for glaucoma and may correlate with disease severity [47, 90]. In patients with open angle glaucoma, more significant field loss tends to occur in the eye with the thinner cornea [91]. Dueker et al. have concluded that CCT is a risk factor for progression from ocular hypertension to POAG. Measurement of CCT is an important component of a complete eye exam, particularly if assessing patients with a risk of developing POAG. Evidence supporting the necessity of measuring CCT as part of screening for POAG or as a risk factor for glaucoma progression is not as strong [92].
Family history has long been known as a risk factor for glaucoma. In the Rotterdam Study, the lifetime absolute risk of glaucoma at age 80 was 10 times higher for individuals having relatives with glaucoma [39]. The Barbados Family Study of open angle glaucoma, looking at inheritance of glaucoma in black families, found family history to be a significant risk factor for development of glaucoma [93].
Martus and Stroux et al. looked at predictive factors for progressive optic nerve damage in glaucoma. In patients with elevated intraocular pressure, significant predictive factors for eventual progression were older age, advanced perimetric damage, smaller neuroretinal rim, and larger area of beta zone peripapillary atrophy [94]. Budde has also studied zone beta peripapillary atrophy in glaucoma patients and has concluded that it enlarges during follow-up in relatively few glaucoma patients. In refractive ranges above minus 3 diopters, enlargement of the beta zone occurs more frequently in progressive glaucoma than in nonprogressive glaucoma. He concluded that in view of its low frequency, enlargement of the beta zone may not be a useful marker for glaucoma progression. Enlargement of peripapillary beta zone was seen in 2.7 % of glaucomatous eyes over 1.5 years. Enlargement of beta zone was observed in 4.4 % of progressive glaucoma eyes versus 2.2 % of stable glaucoma eyes. Finally, excluding eyes over minus 3 diopters, enlargement of beta zone occurred in 6.2 % of progressive eyes versus 0.8 % of stable eyes [95]. In the Beijing Eye Study, the beta zone of peripapillary atrophy was significantly larger and occurred more frequently in glaucomatous eyes than in normal eyes of Chinese adults. No marked difference was noted between chronic open angle glaucoma and primary angle closure glaucoma [96].
Additional reported risk factors have included hypothyroidism and Helicobacter pylori. A study by Girkin at the Veterans Affairs Medical Center in Birmingham, Alabama, found a greater risk of patients with a prior diagnosis of hypothyroidism developing glaucoma [97]. Kountouras et al. identified a relationship between H. pylori and glaucoma [98]. However, these results were refuted by Galloway et al. who found seropositivity for H. pylori was higher in patients with glaucoma (26 %) than in controls (20.2 %), but this difference was not statistically significant [99].
Sleep apnea has been associated with open angle glaucoma. In one study, 114 white patients were consecutively referred for polysomnographic evaluation of suspected sleep apnea syndrome (SAS). Sixty-nine of 114 patients had SAS. Three patients had POAG, while two had normal tension glaucoma. The incidence of glaucoma was 5 of 69, or 7.2 %, which was significantly higher than the expected 2 % incidence in the white population [100]. Geyer and Cohen et al. found no difference in incidence of glaucoma in SAS (2 %) and the general Caucasian population (1.7 %) [101]. POAG was present in 5 of 228 study patients. Although several studies suggest an association between SAS and glaucoma, many are case studies [102–105] and others have low sample size [106–108]. A large population report found a higher incidence of glaucoma in sleep-disturbed patients with breathing disorders compared to normal-sleeping individuals, although the study was based on a questionnaire rather than polysomnographic data [109].
The recent Canadian Glaucoma Study (CGS) focused on systemic risk factors important to the progression of OAG. Investigators followed 258 patients for 5 years, and they identified four independent risk factors that were associated with glaucomatous visual field progression. Despite attempts to minimize the importance of intraocular pressure, it was identified as a significant risk factor for visual field progression. Other risk factors included baseline age, female sex, and abnormal baseline anticardiolipin antibody (ACA). The latter was associated with an almost fourfold increase in glaucoma progression as opposed to normal baseline ACA levels. Patients with diabetes, hypertension, cardiovascular disease, and migraine did not have an increased progression rate [110]. The risk factors are summarized in Table 12.3.
Table 12.3
Risk factors for progression of OAG in the Canadian Glaucoma Study
Risk factor | Hazard ratio |
|---|---|
Abnormal baseline anticardiolipin levels | 3.86 |
Higher baseline age | 1.04 per year |
Female sex | 1.94 |
Higher mean follow-up IOP | 1.19 per 1 mmHg |
An evidence-based assessment of glaucoma risk factors by Friedman et al. has concluded that although many risk factors have been reported, the risk factors most strongly supported by the literature include higher IOP, greater cup to disc ratio, thinner central corneas, and older age. Black race does not appear to be an independent risk factor, although black individuals tend to have thinner corneas, larger cup to disc ratios, and higher IOP, which do have strong associations with POAG [111]. The various risk factors are summarized in Table 12.4. When assessing these risk factors in a particular patient, it is important to remember that risk models should not replace clinical judgment. The clinician must take into account life expectancy, patient health, costs, side effects of treatment, and patient preference when deciding to initiate or change glaucoma therapy.
Table 12.4
Summary of risk factors for diagnosis or progression of glaucoma
Increased IOP |
Older age |
Greater cup to disc ratio |
Thin CCT |
Sex |
Ethnicity |
IOP reduction |
Optic disc hemorrhages |
Antihypertensive use |
Exfoliation syndrome (cause of secondary open angle glaucoma) |
Pigment dispersion (cause of secondary open angle glaucoma) |
Myopia |
Increased disc diameter |
Increased cup to disc ratio (may be a result of the disease process rather than a risk factor) |
Diurnal fluctuationa |
Intervisit fluctuationa |
Decrease systolic perfusion pressure |
Lower systolic blood pressure |
Vascular and/or cardiac diseasea |
Nocturnal blood pressure dip |
Family history of glaucoma |
Peripapillary atrophy |
Hypothyroidisma |
H. pylori a |
Sleep apneaa |
Anticardiolipin antibody |
Hypertension |
Diabetesa |
Cardiovascular disease |
Migraine |
Raynaud’s |
Corticosteroids |
Cholesterol-lowering medications (protective) |
Exercise (protective) |
Elevated venous pressurea |
Compliance/adherence/persistence with treatment |
Smokinga |
Fat intakea |
Older age as a risk factor may simply represent a longer time exposure to the other risk factors. Sex is a weak risk factor. Men have been noted to have an increased risk of disease as well as progression compared to women [112]. Ethnicity as a risk factor may more simply represent an individual’s genetic makeup. Blacks are more prone to glaucoma than any other race. The disease tends to appear at an earlier age and more often leads to blindness [6, 10]. Other studies have demonstrated an increased risk of glaucoma in southern Indians, as well as Hispanic Americans [7, 16, 21, 113].
A higher incidence of glaucoma in myopia may relate to myopes accessing eye care due to their need for glasses. However, an Australian study did show an increased risk of glaucoma in both mild and moderate myopes [114]. Cup size and disc hemorrhage have been described as risk factors for glaucoma. They may be signs of glaucomatous injury rather than actual risk factors. The Baltimore Eye Study found that diabetic patients had higher intraocular pressures, but they did not have on increased risk of glaucoma [115].
Pressure elevation with corticosteroids is a well-known side effect. Cholesterol-lowering agents may be protective with respect to glaucoma [116]. A more recent study by Stein and others found that statin use reduced both the risk of developing open angle glaucoma and progression from glaucoma suspect to open angle glaucoma [117]. Aerobic exercise can lower intraocular pressure in ocular hypertensives [118].
Clinical Assessment
Primary open angle glaucoma is indeed the “sneak thief of sight,” because it is almost always insidious, slowly progressive, and pain-free. Patients are typically unaware that they have the disease, as central vision is impacted only late in the course of the disease. It is typically bilateral but can be asymmetric. Progressive loss of peripheral, paracentral, and central visual fields can lead to blindness. While normal patients have diurnal fluctuations in pressures of 2–6 mmHg, glaucoma patients can have much wider swings in pressure. The highest pressures in most patients are either in the early AM hours or upon awakening. However, some patients have their highest pressure in the afternoon. Some patients are able to tolerate high pressures without sustaining optic nerve damage. Others develop optic nerve injury despite apparently normal intraocular pressures. Further, because an office visit is just one moment in time, it is a poor representation of the maximum IOP that may occur outside the office time frame. Thus, IOP alone cannot be used to make the diagnosis of POAG. The physician should also meticulously inspect the optic nerve head and associated retina nerve fiber layer. Imagine analysis devices (such as HRT, GDx, and OCT) may be useful to supplement direct visualization of the retina by the examiner. Visual field testing should be obtained as well to determine functional loss of vision.
Gonioscopy is essential in the evaluation of all glaucoma suspects and patients (see Figs. 12.5, 12.6, and 12.7). A non-gonioscopic, slit lamp angle grading system was devised by van Herick [119]. The angle between the observation system and the slit beam of the slit lamp is set at 60°. The slit beam is oriented vertically and positioned at the corneal limbus. The peripheral anterior chamber depth is then compared to corneal thickness to estimate the depth of the anterior chamber. Angles are graded one through four, with grade one (shallow) consisting of an anterior chamber depth less than one-fourth of the corneal thickness and grade 4 (deep) being an anterior chamber depth greater than or equal to the corneal thickness. The van Herick grading system is good for suspecting narrow angles but is not a substitute for gonioscopy, which should be performed during the initial assessment of all glaucoma suspects and patients. Periodic reevaluation should be performed as well, especially when confronted with a sudden elevation of pressure, shallowing of the anterior chamber, use of miotics, older hyperopes, cataract progression, or retinal vascular disease. Various angle grading systems exist for describing gonioscopic findings. In some systems where angles are graded 0–4, a grade 4 angle is wide open, while in other grading scales, a “4” may be a closed angle. The Shaffer gonioscopic classification system graded angles from Grade 0 representing a closed angle to Grade 3–4, consistent with a wide open, 20–45° angle where closure is impossible [120]. The Scheie classification system also graded angles as Grade 0 through Grade IV. In Grade 0 all structures of the angle are visible. In Grade I, it is difficult to see over the iris root and into the angle recess. With Grade II, the ciliary body is obscured. Grade III has an obscured posterior trabeculum, and finally Grade IV allows only visualization of Schwalbe’s line [121]. This latter method eliminates the potential confusion of numerical grading systems.



Fig. 12.5
Two of several available gonioscopy lenses. (left) A Zeiss-style 4-mirror lens that couples to the eye with the patient’s own tear film and (right) a Goldmann-style 3-mirror lens that requires Goniosol to couple with the patient’s eye
Fig. 12.6
Zeiss-style 4-mirror lens on the eye of a patient
Fig. 12.7
Goldmann-style 3-mirror lens on the eye of a patient
The American Academy of Ophthalmology has established Preferred Practice Pattern (PPP) guidelines [122]. Each recommendation is written on the basis of three principles: (1) each guideline is clinically relevant and detailed such that is it useful to eye care providers, (2) each guideline is given a rating relative to its importance in the care of the patient, and (3) each guideline is given a rating with respect to the strength of supporting evidence. It should be emphasized that the PPP guidelines provide a template for the general practice of eye care but are not guidelines for the care of all individual patients. The initial exam history should contain an ocular history, a general medical history, a family history, a prior records review, and assessment of the impact of the patient’s visual function in relation to hobbies, employment, and daily living.
The primary ocular examination should include visual acuity; pupillary evaluation; slit-lamp examination; IOP measurement; pachymetry; gonioscopy; stereoscopic evaluation of the optic nerve head and retinal nerve fiber layer; color stereophotography or computer-generated image analysis, preferably dilated fundus examination; and visual field testing.
When therapy is needed, the PPP recommendation is to set a target pressure 20 % less than the mean of multiple IOP measurements and less than or equal to 24 mmHg. I initially shoot for a drop of 30 % from untreated baseline and IOP less than or equal to 21 mmHg. The treatment regimen not only should lower the IOP to the target pressure but should be based on maximal effectiveness and tolerance. Follow-up exam histories should include the ocular history and medical history, with any updates since the last exam. Side effects of treatment medications should be noted. When appropriate, glaucoma medications, including frequency and time of last instillation, should be recorded. Compliance, or adherence, information should be obtained. Although it is frequently misleading, many patients will honestly volunteer that they missed their last dose or they miss multiple instillations during exam intervals. For example, a patient with IOP higher than the target pressure who admits to not using their glaucoma medications the prior evening or that morning may not require a medication change or addition but simply counseling to improve compliance.
PPP follow-up eye exams include visual acuity, slit lamp exam, IOP measurement including time of the day, and gonioscopy when indicated. Patient education is an important component of treatment. This would include discussion of the following: risk factors, long-term prognosis, therapy as well as the need for long-term treatment, therapeutic alternatives including risks and benefits, training on drop instillation including punctal occlusion, and potential side effects of medications.
Frequency of examinations and testing is included in the AAO’s PPP. Suspects may be followed as infrequently as every 12–24 months. At the other extreme, the follow-up interval for uncontrolled glaucoma patients, i.e., target IOP not achieved with high risk of damage, is 4 months or less. My approach has been to follow suspects annually, well-controlled patients every 6 months, and high-risk patients every 3 months. I have summarized my follow-up approach in Table 12.5. The PPP for testing of the optic nerve and visual field is every 3–24 months depending on treatment, whether target IOP is achieved, and risk of damage. In most instances, I get this testing once a year. However, if changes are noted, such as increased cupping, I may get visual field testing and documenting photos more often.
Table 12.5
Recommended frequency of examinations in glaucoma suspects and glaucoma patients with various levels of disease, control, and adherence
Level of glaucoma, control, and adherence | Follow-up |
|---|---|
Suspect | Every 6–12 months depending on risk factors |
Mild, good control, and adherence | 6 months |
Mild, poor control, and/or adherence | 3 months |
Moderate, good control, and adherence | 3–6 months |
Moderate, poor control, and/or adherence | 3 months |
Advanced, good control, and adherence | 3 months |
Advanced, poor control, and/or adherence | 3 months or more frequent |
Quigley has studied practice patterns and found that physicians varied dramatically in their adherence to Preferred Practice Patterns (PPP), performing IOP measurements, disc evaluations and imaging, and visual field tests on 90 % of OAG patients. These same ophthalmologists carried out gonioscopy, CCT measurement, and setting of target IOP in only half of their patients [123].
Another recent study by Fremont et al. assessed conformance of patterns of care for primary open angle glaucoma with American Academy of Ophthalmology’s Preferred Practice Patterns [124]. Most elements of care during initial evaluations of POAG and follow-up visits were performed, including visual acuity examination, intraocular pressure check, slit lamp examination, evaluation of the optic nerve head or nerve fiber layer, and fundus evaluation. However, frequency of other recommended processes fell woefully short. Gonioscopy was performed less than 50 % of the time, optic nerve head drawing or photograph took place just over 50 % of the time, and target pressures were documented 1.3 % of the time. Failure to set a target pressure is worrisome, as future therapy is dependent on whether the intraocular pressure is above or below this target. Intervals between visits followed the Preferred Practice Patterns. An increase in therapy was implemented in less than half the visits where IOP exceeded 25 mmHg. Intervals between visual fields were often surprisingly long. The study concluded that POAG is often undertreated.
Glaucoma should be considered in any patient undergoing an eye exam who has a family history of glaucoma. Glaucoma is more likely when a first degree relative is affected and it is inherited more strongly through the female line. Clinically, glaucoma should be suspected if the intraocular pressure is elevated above 21 mmHg (although as we have seen, glaucoma may occur both above and below statistically “average” IOPs), if the cup to disc ratios are greater than 0.5, or if the cup to disc ratios are asymmetrical by 0.2 or more.
The ophthalmologist should carefully examine the optic nerve head, looking for increased or progressive cupping (Figs. 12.8, 12.9, and 12.10), vertical elongation of the cup (Figs. 12.11, 12.12, 12.13, 12.14, 12.15, 12.16, 12.17, and 12.18), nerve fiber layer hemorrhages (Figs. 12.12, 12.19, and 12.20), nerve fiber layer thinning (Figs. 12.15 and 12.21), peripapillary atrophy (Fig. 12.17), and baring of the optic disc vessels. Any of these findings should alert the eye doctor to initiate appropriate testing and, if indicated, therapy. Broadway and Drance et al. have thoroughly described the evaluation of the optic disc in glaucoma, coming up with four types of discs. Type 1 is the focal glaucomatous disc, with polar or focal notching as well as progressive notch enlargement. Type 2 is the myopic glaucomatous disc. Type 3, or senile, sclerotic optic discs, may show a moth-eaten neuroretinal rim, saucerization, peripapillary atrophy and choroidal sclerosis, and pallor. Finally, the fourth type of glaucoma disc has generalized enlargement of the optic disc cups. Findings may include concentric atrophy, temporal unfolding, extensive notching, or retinal nerve fiber layer atrophy. Other features of the optic disc in glaucoma include cup deepening, neuroretinal rim slope steepening, optic disc margin hemorrhages, pallor/cupping discrepancy, baring of a circumlinear vessel, retinal nerve fiber layer defects, and peripapillary atrophy [125].
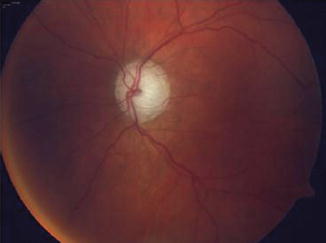

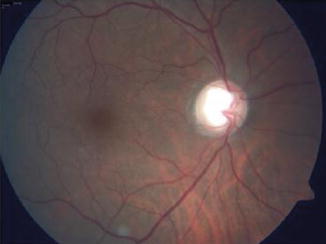
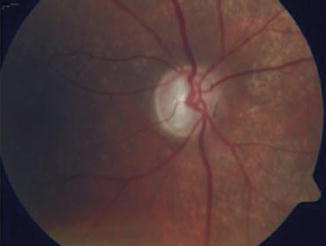

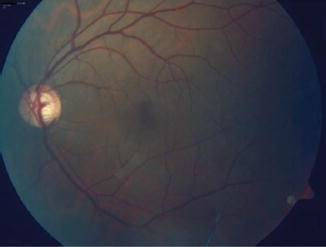

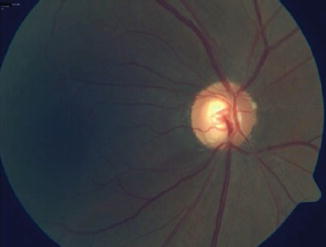
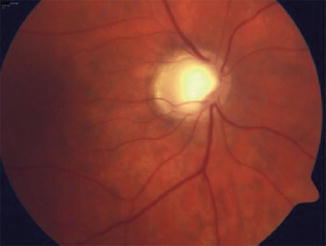
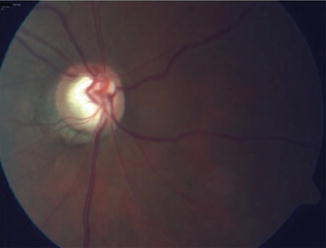

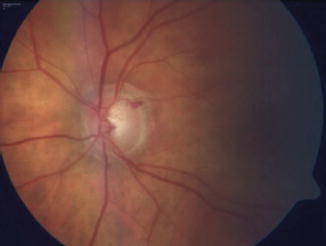
Fig. 12.8
Generalized enlargement of the cup in a patient with advanced glaucoma
Fig. 12.9
Generalized enlargement of the cup in a patient with glaucoma
Fig. 12.10
Generalized enlargement of the cup in a patient with advanced glaucoma
Fig. 12.11
Vertical elongation of cup with thin rim superiorly and inferiorly in advanced glaucoma
Fig. 12.12
Vertical elongation of cup with thin rim inferiorly and a small nerve fiber layer hemorrhage inferiorly
Fig. 12.13
Vertical elongation of cup with thin rim inferiorly
Fig. 12.14
Vertical elongation of cup with thin rim inferiorly
Fig. 12.15
Vertical elongation of cup with thin rim inferiorly and inferior temporal nerve fiber layer loss
Fig. 12.16
Vertical elongation of cup with thin rim inferiorly in Caucasian patient with advanced open angle glaucoma
Fig. 12.17
Vertical elongation of cup with thin rim inferiorly in patient with advanced glaucoma, peripapillary atrophy is present as well
Fig. 12.18
Vertical elongation of cup with thin rim inferiorly
Fig. 12.19




Nerve fiber layer hemorrhage with thin rim superiorly
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
