Skull base defects and injuries are rare, but may occur during endoscopic sinus surgery, as a result of facial trauma, or as a result of tumors in the anterior cranial fossa. Injury to the skull base can lead to catastrophic outcomes such as meningitis, brain abscess, neurological deficits, brain hemorrhage, and death. The content presents ways in which a surgeon may work to prevent or minimize injury to the skull base and describes management of skull base injuries when they do occur, reviews the current literature, and describes various reconstruction techniques used in free tissue grafts and pedicled grafts.
Skull base defects and injuries are rare, but may occur during endoscopic sinus surgery, as a result of facial trauma, or as a result of tumors in the anterior cranial fossa. Iatrogenic injuries resulting in CSF leaks through skull base defects have been noted to have an incidence of 0.46% to 0.85%. Injury to the skull base can lead to catastrophic outcomes that include meningitis, brain abscess, neurologic deficits, brain hemorrhage and death. This content discusses ways in which a surgeon may work to prevent or minimize injury to the skull base. We also describe management of these injuries when they do occur, review the current literature, and describe various reconstruction techniques.
Prevention
If unrecognized, anatomic variations may contribute to surgical complication along the anterior skull base. One such anatomic variation that may occur along the ethmoid roof is described by the Keros classification, which measures the vertical height between the cribriform plate and the fovea ethmoidalis ( Table 1 ). In this classification, the depth of the olfactory fossa is categorized as 1 to 3 mm (Keros I), 3 to 7 mm (Keros II), or 7 to 16 mm (Keros III). As the bone in this region is typically quite thin, increased vertical height lends itself to increased vulnerability. In Keros’ original study of 450 cadavers, 12% were found to be Keros I, 70% Keros II, and 18% Keros III. This proportion has been supported by several recent CT studies. Also notable in recent studies has been asymmetry of greater than 2 mm in 8% of patients ( Fig. 1 ).
| Classification | Depth of the Olfactory Fossa |
|---|---|
| Type I | 1–3 mm |
| Type II | 3–7 mm |
| Type III | 8–16 mm |
| Asymmetric | Asymmetric |

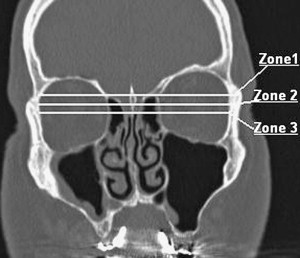
Pre-operative CT scans may also be evaluated for the presence of a low-lying skull base. Meyers and Valvassori found that a horizontal line drawn along the roof of the ethmoid passed above the vertical mid-point of the orbit in 88% of the cases studied. Approximately 10% of cases crossed the orbit at the vertical midplane and 2% of cases were below the vertical midplane. Stankiewicz and Chow built on this data from Meyers and Valvassori’s study to develop safety zones based on the relationship of the skull base to the level of the orbit. Fig. 2 depicts this concept with zone 1 being the safest. When the horizontal line drawn from the roof of the ethmoid crosses the upper one-third of the orbit, this is considered the most safe anatomic arrangement. Caution is to be used in cases in which the ethmoid roof crosses below the midplane of the orbit.
Other anatomic considerations when working along the skull base include the extent of sinus disease. Extensive disease can affect visualization during surgery due to increased inflammation and consequent intra-operative bleeding. Intra-operative bleeding has been noted to be significant in several case series that discussed iatrogenic skull base injuries, and this bleeding may be related to the extent of inflammation and sinus disease. On the other hand, DelGaudio and colleagues found that 74% of skull base injuries occurred in patients with minimal or no mucosal disease. They postulated that injury was a result of less resistance and thinner bone in the less diseased sinuses. Diseased sinuses may have thicker bone as a result of sinus oteoneogenesis.
Use of powered instruments, such as the microdebrider, are commonplace in the surgical management of sinus disease. A microdebrider suctions while a rotating blade cuts through the tissue suctioned into the device. Consequently, a significant amount of tissue can be removed quickly. Due to this aggressive cutting nature, a microdebrider should be used very judiciously along susceptible areas such as the skull base. Surgeons may consider using through biting instruments and grasping instruments in these more vulnerable areas. One must always remember that injuries can occur regardless of instrument or technique.
There are two differing approaches when performing sinus surgery. Messerklinger advocated surgery that involved the anterior ethmoid cavities. He did not advocate aggressive surgical dissection beyond the anterior ethmoid for he felt that the larger sinuses improved when the ventilation of these sinuses improved with the ethmoidectomy. As a result, the surgery is often performed in a front to back technique. Alternatively, Wigand describes performing surgery in a back-to-front approach. This technique may allow for easier identification of the skull base earlier in the procedure. We favor this approach in sinus surgery since there is early identification of the skull base, and we believe that the downward angle of the skull base favors a posterior to anterior dissection as a means to avoid inadvertent penetration of the skull base.
Institutions throughout the country train hundreds of residents annually. Close supervision is paramount in sinus surgery. Bumm and colleagues reported the most injuries occurred performed by surgeons in the second half of their residency. These surgeons had performed between 100 and 300 sinus surgeries and typically were unsupervised until the end of the case. The study concluded that this particular group of trainees had enough training to feel falsely safe. This study also noted a difference in location of injury. Early in training, the injuries were noted to be at the anterior ethmoid near the medial concha base (lateral lamella, cribriform plate) whereas, skull base injuries with more experienced surgeons were located in the immediate vicinity of the frontal sinus. Institutions that train residents should consider dissection techniques that allow for the largest margin of safe surgery.
Image guided systems are used regularly in the operating room. When using image guidance, the surgeon should understand the target recognition error (TRE) implicit in this technology. TRE is defined as the location of targets interest compared with the corresponding locations on CT scan. It will vary depending on the position as it relates to the fiducial. Labadie and colleagues concluded that the TRE was approximately 2 mm. Therefore, this technology functions with a built-in margin of error, and is not a substitute for an in-depth understanding of sinus and skull base anatomy. Meticulous registration and cross checking of the instruments will improve accuracy, however, it is imperative that the surgeon not over rely on the accuracy of the device.
Having a surgical plan with each operation is important. Mapping out a plan of action with a pre-operative CT scan may lessen the likelihood of injury. On a CT scan, the Keros classification, length, height and slope of the skull base, asymmetry of the cribriform plate, and dehiscence of bony structures should be evaluated before surgery. By performing this review with each patient’s CT preoperatively, one may develop an increased understanding of which particular anatomic abnormalities to expect during surgery.
Management of skull base injury
If a skull base injury occurs, the defect should be thoroughly assessed. If evaluated in a post-operative setting, the assessment should include nasal endoscopy. Collection of the rhinorrhea for beta-2 transferrin can confirm a true CSF leak. A preoperative CT scan can help detect the extent of the injury and localization when done in thin slices (1 mm) with coronal and sagittal reconstructions. Often an MRI is performed to assist in diagnosing the contents that have herniated through a defect. Other methods such as radio-nuclide scanning and CT cisternograms may be useful in diagnosis, although we have found their usefulness to be limited.
Intraoperative use of intrathecal fluorescein has been associated with severe complications such as lower extremity weakness, numbness, generalized seizures, opisthotonus, and cranial nerve deficits. Caution must be taken when using intrathecal fluoroscein due to these risks. It may be useful in spontaneous CSF leaks or radiographically non-apparent skull base defects. Several studies have advocated its use with no reported adverse outcome. Using the lowest possible concentration is therefore recommended.
Jones and colleagues described a novel use of fluroscein in 1990. They topicalized 10% fluoroscein which is initially yellow and diagnosed the CSF leak with a color change of the fluoroscein that turned green when in contact with CSF. This eliminated the need for intrathecal fluoroscein and eliminated the risks involved with its use. Saafan and colleagues confirmed the efficacy of this technique in diagnosis of CSF leak in their series of 25 patients. The most common site of leakage in this study was the ethmoidal roof (52%). There were five iatrogenic injuries but the study did not specify the location of the iatrogenic injuries. Their conclusion advocated the use of this technique preoperatively, intraoperatively, and postoperatively. Other studies have also categorized the location of the skull base defects. Tables 1–3 show the distribution of skull base defects by location and etiology, respectively.
| Study | N | Cribriform | Ant Eth | Post Eth | Frontal | Sphenoid |
|---|---|---|---|---|---|---|
| Banks et al e | 193 | 32 | 64 a | – a | 23 | 64 |
| Harvey et al | 106 | 15 | 19 a | – a | 7 | 62 d |
| Lee et al | 39 | 13 | 11 | 5 | 3 | 7 |
| Zuckerman et al | 42 | 9 | 14 a | – a | 2 | 17 |
| Bumm et al | 32 | 14 | 3 | – b | 6 | 7 b |
| Briggs and Bolger | 20 | 9 c | – c | – c | 3 | 8 |
| Zweig et al | 53 | 19 | 15 a | – a | 0 | 20 |
a Study did not differentiate anterior and posterior ethmoid.
b Study grouped posterior ethmoid defects with sphenoid defects.
c Study grouped cribriform plate, anterior ethmoid and posterior ethmoid defects.
d Study separated CSF leak from sella as a separate location.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


