Preoperative Issues
Rupal H. Trivedi
M. Edward Wilson
A thorough preoperative evaluation sets the stage for the decision making that precedes surgery.1 A comprehensive history and an ocular and systemic examination help the care team to plan the overall management of the child with a cataract. The goals of the preoperative assessment include deciding whether surgery is needed, and if needed, what the appropriate timing of the surgery is. In addition, the characteristics of the cataract are documented and the postoperative visual prognosis estimated. During the assessment, we also often gain insight into whether the child and the family will comply with the postoperative correction of residual refractive error and amblyopia treatment. These data, together, help us decide whether it is best to implant an intraocular lens (IOL) or not, and if implanted, what postoperative refractive error should be aimed for when selecting an IOL power.
IMPORTANT DECISIONS
During history taking and examination, the physician needs to make several important decisions. Among these are whether surgery is indicated or not, and if indicated, how to handle aphakic rehabilitation, etc.
Indication for Surgery
The surgeon should be careful to operate on only those cataracts where the visual disturbance is severe enough to justify sacrificing normal youthful accommodation. Indications for cataract surgery include a cataract that obstructs the examiner’s view of the fundus of the nondilated pupil or a blackened retinoscopic reflex preventing refraction of the patient. Deciding when to remove a partial cataract can be difficult. Nonverbal children add more difficulties to this decision. In each individual case, the ophthalmologist needs to use his or her best judgment about whether a partial cataract is interfering with visual functioning enough to warrant removal. Partial cataracts can be amblyogenic and may disturb emmetropization leading to abnormal axial elongation. For verbal children, cataract surgery is contemplated if Snellen visual acuity (VA) is 20/50 or worse or if the child is intolerant to glare or resistant to amblyopia therapy with documented deteriorating visual function. Since a subjective VA cannot be obtained in infants with cataracts, greater reliance is placed on the morphology of the cataract, other associated ocular findings, and the visual behavior of the child, in order to ascertain whether the cataract is visually significant or not. The degree of visual impairment induced by a lens opacity differs markedly depending on the location of the opacity. Generally, the more posterior and the more central the opacity, the more amblyogenic it is. Generally speaking, a cataract that blackens the retinoscopic reflex for 3 mm or more in the center of the pupil is considered visually significant.
If a partial cataract is being treated conservatively, it is important to carefully follow these children. Conservative treatment using mydriatic drops necessitates the patient’s wearing glasses for reading if any cycloplegic effect is induced. This has not found widespread acceptance. Associated glare and loss of accommodation are the most common obstacles. Visual outcome has also been unimpressive. Despite these limitations, the use of mydriatic drops may be kept in reserve in eyes with slowly progressive cataracts or paracentral cataracts <3 mm and, especially, in patients for whom cataract surgery needs to be deferred for any reason—be it medical (high risk for anesthesia), social, or economical.
Timing of Surgery
Deciding on the appropriate timing of surgery is most critical during early infancy. In the case of a unilateral dense cataract diagnosed at birth, the surgeon can wait until 4 to 6 weeks of age. Waiting until 30 days of age or more decreases the anesthesia-related risks and often allows term infants to be healthy enough for discharge to home after surgery. Premature babies or term infants operated before 30 days of age are usually kept overnight for observation since the incidence of apnea after anesthesia is higher. For dense unilateral cataracts documented to be visually significant at birth, waiting beyond 6 weeks may adversely affect visual outcome.2,3 In the case
of a bilateral cataract diagnosed at birth, a good visual outcome can be achieved if the child is operated before 10 weeks of age.4 The first eye surgery can be offered at 4 to 6 weeks of age, and the second eye surgery after another 1 to 2 weeks’ time. It is important to keep the time interval to a minimum between the two eye surgeries. Some surgeons advise patching the first operated eye until the second has had surgery, to prevent amblyopia in the second operated eye.5 This type of occlusion is not commonly done but undue delays between surgeries should be avoided in infants. For older children, the timing of surgery is not as crucial. In children beyond the amblyopic age, surgery can often be decided based on convenience and other logistical issues.
of a bilateral cataract diagnosed at birth, a good visual outcome can be achieved if the child is operated before 10 weeks of age.4 The first eye surgery can be offered at 4 to 6 weeks of age, and the second eye surgery after another 1 to 2 weeks’ time. It is important to keep the time interval to a minimum between the two eye surgeries. Some surgeons advise patching the first operated eye until the second has had surgery, to prevent amblyopia in the second operated eye.5 This type of occlusion is not commonly done but undue delays between surgeries should be avoided in infants. For older children, the timing of surgery is not as crucial. In children beyond the amblyopic age, surgery can often be decided based on convenience and other logistical issues.
Sequential cataract surgery, more popularly known as immediately sequential bilateral cataract surgery (ISBCS), remains controversial (see Chapter 9). Almost every discussion on ISBCS either starts or ends with a comment on the disagreement surrounding its use. The important question is not “can it be done?” but, more properly, “should it be done?” Even conservative surgeons, who vote against the routine use of ISBCS in children, are more likely to use this approach when anesthesia poses more than average risks or if the patient lives far away and a visit for surgery on the second eye would be difficult.
Timing of surgery in children with traumatic cataract, uveitis, and retinoblastoma is discussed in appropriate chapters (see Chapters 35, 38, and 40).
Aphakic Rehabilitation
IOL implantation in children has the benefit of reducing dependency on compliance with other external optical devices (aphakic glasses and contact lenses) and providing at least a partial optical correction constantly. These are important advantages to the visual development in amblyopia-prone eyes. However, concerns about primary IOL implantation are the technical difficulties of implanting an IOL in the eyes of small children, selecting an appropriate IOL power, and the risk of visual axis opacification (VAO) after implantation in the very young.6 On the other hand, although it is possible for an eye with a unilateral infantile cataract to achieve a good visual outcome following contact lens correction, it requires cooperation from children. Both IOLs and aphakic contact lenses may support similar VA after surgery for unilateral cataract in the presence of good compliance with contact lens. However, IOLs support better VA when compliance with contact lens wear is moderate or poor.7 For bilateral cataracts, aphakic glasses or contact lens use are reasonable options. Infant aphakia treatment study6 concluded that until longer-term follow-up data are available, caution should be exercised when performing primary IOL implantation in children aged 7 months or younger given the higher incidence of adverse events and the absence of short-term visual outcome compared with the contact lens use. For children beyond infancy, IOL implantation is less controversial and more commonly employed.
HISTORY
Parent/caregivers may present with a chief complaint of noticing a white spot in the child’s eye (Fig. 5.1A-C), visual inattentiveness, nystagmus, strabismus, asymmetry of one eye relative to the other (e.g., microphthalmos), photophobia, ocular injury, or simply because of referral from other physician who has identified a possible lens opacity. At times, the evaluation is scheduled because of a family history of childhood cataracts or because the child has one of a growing number of systemic conditions or syndromes that can be associated with cataracts. Specific information is gathered on gender, ethnicity, and date of birth; birth weight; evidence of maternal infection (especially the TORCH infections), rash or febrile illness during pregnancy (may be suggestive of intrauterine infection), any other prenatal and perinatal history that may be pertinent (e.g., alcohol, tobacco, drug use, ionizing radiation during pregnancy), history of ocular trauma (unless cataract appears to be purely nontraumatic), age at onset of visual symptoms, ocular status on previous eye examinations (can be helpful in assessing visual prognosis after treatment), and history of corticosteroid therapy (especially in posterior subcapsular cataract [PSC]).1 Simple questions can help in determining the surgical need, the timing or urgency of surgery, and the visual prognosis after cataract removal (e.g., Does your child appears to see well? Do your child’s eyes look straight or do they seem to cross or drift or seem lazy? How long have you noticed a change in your child’s visual function?). Frequently, even with poor vision, a child may be functioning reasonably well in a familiar environment. The child will be reluctant, however, to explore an unfamiliar area. Ask parents how well their child functions in a new environment, which is a useful indicator of vision. Infants with complete bilateral congenital cataracts usually demonstrate decreased visual interest and experience delayed milestones.
Approximately one-third of cataracts are inherited, so family history of childhood cataract should be evaluated (especially in bilateral cataract). Mention to the parents that you may want to look at their eyes (Fig. 5.2). Explain that a finding in the eyes of the parents may help streamline the evaluation and workup of the child, thus preventing unnecessary tests.
EXAMINATION
Art of Examining Children
A friendly manner, a little trickery, and a lot of praise are essential elements in the art of examining children.8 Pediatric exam is not as methodical and sequenced as the adult exam. Since children are not merely small adults,
the temptation to proceed methodically and sequentially through each portion of the complete eye exam in each patient needs to be resisted. Remember that the doctor does not decide when the exam is over, the child does. Use the limited attention span and cooperation of the child to perform the investigations most essential. If child is not cooperative in office, most examinations can be performed during examinations under anesthesia (EUA) before surgery. The doctor’s initial behavior should be aimed at establishing trust. The doctor should be seated, so as not to stand over the child. Invite the child to sit in the BIG chair on a parent’s lap or alone. Raise the chair quickly so that the child is at least at eye level with everyone in the room. Don’t surprise the child. Talk directly to the child. For older children, comment on his or her clothing or ask a question you know he/she can answer, such as: How old are you? What grade are you in? What are you doing this summer? When a child begins to speak, his/her anxiety level drops dramatically. It is also helpful to show the child a toy and let the child hold it. Tell the child what to do. Be animated. Have colorful toys. Whistle, make noises, and call the child by name. Use an age-appropriate vocabulary (e.g., Phoropter = elephant glasses). During the course of the exam, pause whenever you need a break or the child “demands” one. Remember, the child and parent will detect any hint of frustration in your voice. Praise children for being “grown-up,” for doing great, and for having amazing eyes. Throw a few “almost done” comments to keep them cooperative. More praise can be done at the end, even if they did not do as well as you hoped. Patients with pediatric cataract require repeated follow-up examinations. It is important to have the child feel reasonably good about the clinic visit, which may help during the next clinic visit.
the temptation to proceed methodically and sequentially through each portion of the complete eye exam in each patient needs to be resisted. Remember that the doctor does not decide when the exam is over, the child does. Use the limited attention span and cooperation of the child to perform the investigations most essential. If child is not cooperative in office, most examinations can be performed during examinations under anesthesia (EUA) before surgery. The doctor’s initial behavior should be aimed at establishing trust. The doctor should be seated, so as not to stand over the child. Invite the child to sit in the BIG chair on a parent’s lap or alone. Raise the chair quickly so that the child is at least at eye level with everyone in the room. Don’t surprise the child. Talk directly to the child. For older children, comment on his or her clothing or ask a question you know he/she can answer, such as: How old are you? What grade are you in? What are you doing this summer? When a child begins to speak, his/her anxiety level drops dramatically. It is also helpful to show the child a toy and let the child hold it. Tell the child what to do. Be animated. Have colorful toys. Whistle, make noises, and call the child by name. Use an age-appropriate vocabulary (e.g., Phoropter = elephant glasses). During the course of the exam, pause whenever you need a break or the child “demands” one. Remember, the child and parent will detect any hint of frustration in your voice. Praise children for being “grown-up,” for doing great, and for having amazing eyes. Throw a few “almost done” comments to keep them cooperative. More praise can be done at the end, even if they did not do as well as you hoped. Patients with pediatric cataract require repeated follow-up examinations. It is important to have the child feel reasonably good about the clinic visit, which may help during the next clinic visit.
 Figure 5.1 A-C. Cataract presented as white reflex. (Reprinted from Trivedi RH, Wilson ME. Pediatric cataract: preoperative issues and considerations. In: Wilson ME, Saunders RA, Trivedi RH, eds. Pediatric Ophthalmology: Current Thought and a Practical Guide. Berlin, Heidelberg: Springer, 2009, with permission.) |
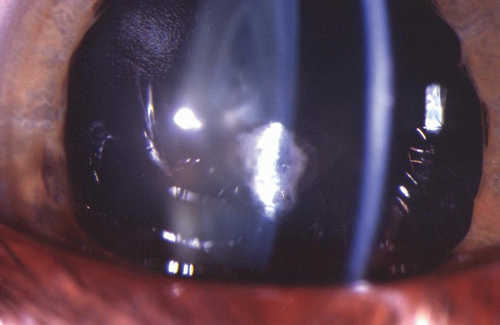 Figure 5.2. Unoperated cataract observed in mother’s eye. The child was operated for cataract. (Reprinted from Trivedi RH, Wilson ME. Pediatric cataract: preoperative issues and considerations. In: Wilson ME, Saunders RA, Trivedi RH, eds. Pediatric Ophthalmology: Current Thought and a Practical Guide. Berlin, Heidelberg: Springer, 2009, with permission.) |
Children dislike the drops and they can get cranky after waiting for dilated eye examination. We do dilated eye examination during EUA just before surgery. If pupil dilation is needed in the clinic, have someone other than the examiner place the drops and make sure they are preceded with a topical anesthetic. This too can be done
quickly so the child can be consoled by the parent and can retreat to the comfort of a playroom or a toy-filled sub-waiting area. If fundus examination is done in the clinic, it helps to convey to children that you are putting on a “strange hat” that can look all the way into their “brains.” Then as you view the optic nerve and macula, praise the children for being smart since they have “lot of brains.” Be efficient by getting the look you need as quickly as possible. Pediatric eye exams are done as a team. The need to see more patients in less time has eliminated the luxury of having the pediatric ophthalmologist perform the entire exam him/herself. Pediatric ophthalmology is no longer a solo sport; it is a team game. Train the team so that everyone adopts the same child-friendly habits.
quickly so the child can be consoled by the parent and can retreat to the comfort of a playroom or a toy-filled sub-waiting area. If fundus examination is done in the clinic, it helps to convey to children that you are putting on a “strange hat” that can look all the way into their “brains.” Then as you view the optic nerve and macula, praise the children for being smart since they have “lot of brains.” Be efficient by getting the look you need as quickly as possible. Pediatric eye exams are done as a team. The need to see more patients in less time has eliminated the luxury of having the pediatric ophthalmologist perform the entire exam him/herself. Pediatric ophthalmology is no longer a solo sport; it is a team game. Train the team so that everyone adopts the same child-friendly habits.
Assessment of Visual Function
The method of evaluating visual function will vary according to the age of the child and the level of cooperation. A communication barrier exists between the ophthalmologist and very young preverbal or preliterate patients.
Parents and caregivers can help to break this communication barrier by working together to encourage the child to perform functional testing in the office that can help quantify the VA of the child with cataract as precisely as possible. Documentation of the child’s level of cooperation with the examination can be useful in interpreting the results and in making comparisons among the examinations over time. When results are equivocal, repeated office visits may be needed. We use an occlusive patch to isolate one eye for VA testing. Children are experts at peaking around an occluder. We tell the child that they can take the patch off as soon as the testing is completed. That seems to comfort them somewhat. They know the patch is temporary.
Infant and Preverbal Child
The assessment strategy is to determine whether each eye can fixate on an object, maintain fixation, and then follow the object into all directions. The assessment should be performed binocularly and then monocularly. This can be done by drawing the child’s attention to the examiner’s or family member’s face (infants under 3 months) or a handheld toy either at 1/3 m or any other measured distance (1 m, 3 m/10 feet, 6 m/20 feet). The force with which the child objects to alternate occlusion of the eyes is useful to judge the relative vision in each eye. Fixation behavior is recorded for each eye as “fixates, follows, maintains.” Some prefer the terms “central, steady, and maintained” to describe the fixation observed. In an awake and alert child, if poor fixation and following are noted binocularly after 3 to 4 months of age, a significant visual loss is suspected, and searched for.
For strabismic children, an assessment of binocular fixation pattern is performed in which the examiner determines the length of time that the nonpreferred eye can hold fixation. It can be reported as will not hold fixation with nonpreferred eye, holds fixation briefly with nonpreferred eye, or no fixation preference. With a straight-eyed child and those with small angle deviation, the base-down prism-induced tropia fixation test can be used to optically separate the two eyes. A 20 prism-diopter base-down prism is our preferred instrument since it displaces the pupillary reflex and the image sufficient to detect which eye is being used for fixation at any time during testing (Fig. 5.3A-C). The prism is placed before one eye at a time for approximately 2 seconds and the fixation response is described. A scoring system can be used where the responses to the base-down prism are noted using a −2 to +2 scale. In this system, the right eye receives the prism first. A score of −2 means that the child fixates with the left eye only, −1 is when the child alternates at times but prefers OS, 0 indicates alternate fixation without preference, +1 means that the child alternates at times but prefers OD, and +2 indicates that the child fixates with the right eye only. The prism is then placed over the left eye, and it is scored using the same scale. The total induced tropia test (ITT) score is the sum of the grades of the right eye and the left eye. Scores of ±3 or ±4 indicate a strong fixation preference and probable poor vision, whereas scores of 0 or ±1 indicate little or no fixation preference and probably better vision. The results of the ITT can be recorded simply as alternates or the preferred eye is the right/left and nonpreferred eye holds well, holds briefly, or shows no hold. However, the quantitative scoring system is helpful to monitor early postoperative surgical outcome and in subsequent amblyopia management.9
In preverbal children with partial cataracts or lamellar cataracts, we also use foot-pedal-operated “barking dogs” or other noise-making and moving toys at the distance within the examination room. Each toy needs to be mounted on a shelf and displaced vertically from one another (Fig. 5.4A-C). As the examiner activates one toy and then another using the foot-pedal switch, the quality of the saccade from the child is noted. At 20 feet, a brisk saccade to the activated toy from the one simultaneously inactivated toy represents sufficient visual function in that eye to place into question the need for surgery on a partial cataract.
Other quantitative methods such as preferential looking techniques (Teller acuity cards or Lea paddles) or Cardiff cards can be used. The Hiding Heidi test by Lea is also useful to detect loss of vision in the lower contrast setting. It works on the preferential looking principle. A sweep visual evoked response can also quantify VA, but it may not always be readily available. Candy sprinkles can be used on a tray to get additional information about the child’s functional vision. If the child can easily find a small candy sprinkle, this illustrates an ability to localize a small object. Watching the child struggle or fail this task can also serve to help verify the significance of the lens opacity.
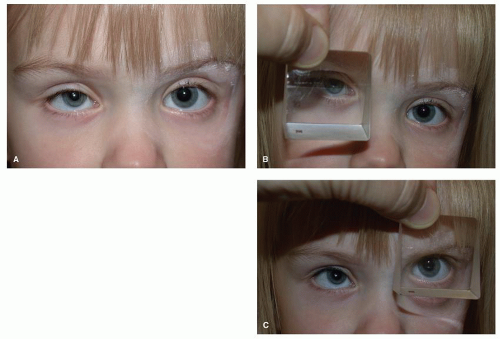 Figure 5.3 A-C. Base-down prism test. (Reprinted from Trivedi RH, Wilson ME. Pediatric cataract: preoperative issues and considerations. In: Wilson ME, Saunders RA, Trivedi RH, eds. Pediatric Ophthalmology: Current Thought and a Practical Guide. Berlin, Heidelberg: Springer, 2009, with permission.) |
Verbal Child
Quantitative VA assessment in cooperative verbal children can be assessed using optotype VA testing (identifying or matching symbols or letters), allowing quantification of VA on a Snellen or preferably, a logMAR scale. Distance VA should be determined monocularly whenever possible. The fellow eye should be completely covered (with adhesive occluder to prevent peeking). The test should
be performed at a distance of 10 to 20 feet with the eye chart calibrated to the exact measured distance from the examination chair to the chart. Children should be tested using a linear display of letters if possible. Young children may be easier to test if isolated optotypes with crowding bars are used. We like the HOTV or the Lea symbols matching game since the letters/symbols can be called by name or identified by pointing to the matching letter/symbol on the lap card.1 The letters HOTV are chosen because they avoid right to left confusion by being mirrorimage letters. In addition to VA, the testing distance, type of optotype, whether the optotype is presented a line at a time or isolated, and cooperation level of the child should be documented in the medical record. If the child returns for repeat testing, the weaker eye should be tested first. Young children have short attention spans and may perform better on the first eye tested and lose interest more quickly on the second eye. Also, when testing VA at near, the testing distance must be controlled precisely. We prefer the HOTV or Lea near chart with a rope attached so that the testing distance can be easily verified and maintained. Other near cards may give falsely good VA measurements when the child leans in and reduces the testing distance to a fraction of the distance to which the chart was calibrated.
be performed at a distance of 10 to 20 feet with the eye chart calibrated to the exact measured distance from the examination chair to the chart. Children should be tested using a linear display of letters if possible. Young children may be easier to test if isolated optotypes with crowding bars are used. We like the HOTV or the Lea symbols matching game since the letters/symbols can be called by name or identified by pointing to the matching letter/symbol on the lap card.1 The letters HOTV are chosen because they avoid right to left confusion by being mirrorimage letters. In addition to VA, the testing distance, type of optotype, whether the optotype is presented a line at a time or isolated, and cooperation level of the child should be documented in the medical record. If the child returns for repeat testing, the weaker eye should be tested first. Young children have short attention spans and may perform better on the first eye tested and lose interest more quickly on the second eye. Also, when testing VA at near, the testing distance must be controlled precisely. We prefer the HOTV or Lea near chart with a rope attached so that the testing distance can be easily verified and maintained. Other near cards may give falsely good VA measurements when the child leans in and reduces the testing distance to a fraction of the distance to which the chart was calibrated.
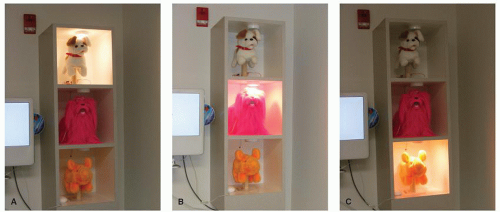 Figure 5.4. A: The upper foot-pedal-operated animal is activated. B: The middle foot-pedal-operated animal is activated. C: The lower foot-pedal-operated animal is activated. (Reprinted from Wilson ME. The art and science of examining a child. In: Wilson ME, Saunders RA, Trivedi RH, eds. Pediatric Ophthalmology: Current Thought and a Practical Guide. Berlin, Heidelberg: Springer, 2009, with permission.) |
Fusion and stereoacuity testing at distance as well as near may also be helpful when deciding how much visual dysfunction is present in a cataract patient. In children with PSCs who complain of intolerable glare, but have good Snellen VA, glare testing should be performed to evaluate the need for surgery.
VA is a useful means of assessing one aspect of visual function, but it provides a very limited indication of the patient’s visual perception. Most objects in the visual scene are not at the high black-white contrasts employed in VA testing. Assessment of the patient’s ability to detect stimuli at lower contrasts is very useful. Tests such as low-contrast test pictures in infancy and childhood provide important information about the distance at which the child can see facial features. Contrast sensitivity measurements can first be performed using the enhancement game, that is, single low-contrast symbols.10 Low-contrast optotype tests are either VA charts at low-contrast or tests with one symbol size at different contrast levels. Individuals with equal VA at high contrast may have different low contrast VA.
Red Reflex Test
The red reflex test can be used to detect the density and extent of the opacity in the visual axis. The retinoscope is a very useful instrument for viewing the red reflex within the pupillary space to see how much of the reflex is blackened by the cataract. In addition, the direct ophthalmoscope can be used to perform the Bruchner red reflex test where both eyes are viewed together and the red reflexes compared. When both eyes are viewed simultaneously, potentially amblyogenic conditions, such as anisometropia, strabismus, and asymmetric cataracts can be identified. The direct ophthalmoscope is focused on both eyes simultaneously at approximately 3 feet away.
Ocular Alignment and Motility
Details on strabismus and nystagmus mainly help when explaining prognosis to the parents and to prepare them for patching or further surgeries. Ocular alignment is assessed by comparing the corneal light reflection of one eye with the other, looking for asymmetry between the eyes using the binocular red reflex test, and by the cover/uncover and alternate cover tests. Cover/uncover and alternate cover tests are performed in primary gaze at distance and at near. Detailed targets that require precise accommodation are utilized when feasible. These tests require the patient’s cooperation and interaction with the examiner in addition to sufficient vision to fixate on the target. Earlier-onset unilateral cataracts have the highest risk for strabismus and late-onset bilateral cataracts have the least risk. Also, as a general rule, patients with partial cataracts and relatively good preoperative VA have less strabismus. Strabismus at presentation is often an indication that the cataract is long standing and that significant amblyopia is likely to be present. Infants with profound bilateral dense cataracts develop nystagmus at approximately 3 months of age because the fixation reflex that normally appears by that time is prevented from developing. Once nystagmus has developed, it is likely to persist even if the cataracts are subsequently removed. On occasion, nystagmus will disappear when surgery is performed within weeks to months after onset of the nystagmus. However, this is the exception rather than the rule. When manifest nystagmus does develop and persist, the visual prognosis is worse. VA in eyes with nystagmus and infantile cataracts is rarely better than 20/100 after cataract surgery.
EXTERNAL EXAMINATION, ANTERIOR SEGMENT EVALUATION, AND OTHER INVESTIGATIONS
External examination of the eye with a suspected cataract usually consists of a penlight evaluation of eyelids, eyelashes, conjunctiva, sclera, cornea, and iris. Evidence of blepharitis (Fig. 5.5) or any discharge or tearing should be evaluated and if applicable, treatment should be advised prior to the proposed surgery date. For pupil—size, shape, symmetry, and reaction to light should be noted. Microphthalmia and poorly dilating pupils are indicators of arrested development and increase the risk of a poor anatomical and functional outcome after cataract surgery. It has been our impression that poorly dilating pupils indicate an overall immaturity of the anterior segment and may be a marker for increased risk of glaucoma after cataract surgery.
 Figure 5.5. Blepharitis in a 6-year-old child scheduled for intraocular surgery. |
After dilation, a slit-lamp evaluation should be carried out if the child is old enough to be cooperative. The slitlamp examination findings can help with the search for a cause of the cataract, help establish a prognosis, and help plan the surgical strategy. The morphology of the cataract may affect prognosis and give a clue to the etiology. Unilateral PSC should prompt a careful search for evidence of trauma. Bilateral PSC cataract may result from chronic uveitis, prolonged corticosteroid treatment for chronic disease, radiation treatment for malignancy, or nonaccidental injury (child abuse). Children with juvenile idiopathic arthritis (JIA) may have associated band-shaped keratopathy and posterior synechia. Lens subluxation, iridodonesis, and aniridia should be looked for. Total cataract involving the whole lens can occur in Down syndrome, type 1 diabetes mellitus, congenital rubella, and posterior lentiglobus. In cases of unilateral cataract, examination of the fellow eye after pupil dilation is essential to rule out asymmetric bilateral findings. Anterior lenticonus is most often associated with Alport syndrome and should be investigated accordingly. A sudden onset of total cataract may be an indication of unsuspected trauma, diabetic cataract, or preexisting ruptured anterior (reported in anterior lenticonus) or posterior capsule (reported in posterior lentiglobus). If the anterior vitreous can be visualized, the “fish-tail” sign suggests that the posterior capsule is incompetent or grossly ruptured. Fish-tail refers to the to-and-fro movement of the lens material in the vitreous as the eye gazes slightly right and left.
For children above about 5 to 6 years of age, the ability of the child to cooperate for slit-lamp examination is also an indirect indicator that the child will cooperate for Nd-YAG laser capsulotomy if needed. In children above 5 to 6 years of age with an intact posterior capsule and an AcrySof® IOL implantation, visually significant posterior capsule opacification (PCO) is known to develop most commonly at 18 to 24 months after surgery. If a child in this age range seems to be cooperative for slit-lamp examination during the preoperative evaluation, the surgeon may decide to leave behind an intact posterior capsule (assuming high odds of getting the child’s cooperation for YAG-laser if needed).
A slit-lamp examination of both parents, if possible, helps to establish the presence of familial cataracts and cataract-associated conditions. These findings can be subtle and the parents may not have been told that they have any pathology at all. Variability of the severity of cataracts within the same family is common.
OCT can be performed preoperatively if the lens is clear enough and the child is able to cooperate (see Chapter 21). Baseline specular microscopy is advised by some; however, it is more commonly used for secondary IOL implantation or anterior chamber IOL implantation.
Axial Length Measurement and Keratometry
For older children, axial length (AL) measurement can be obtained in office using ultrasound or optical biometry. This is especially important if A-scan instrument is not available in the operating room. Similarly, keratometry can be performed in the clinic.
Ultrasound Biometry
The ultrasound probe is placed into the solution and positioned parallel to the axis of the eye. Axiality is judged by watching for the correct spike patterns on the oscilloscope screen as the probe position is adjusted. The examiner should be familiar with the characteristics of a good A-scan tracing with a spike from each layer of the eye. When the probe is aligned with the optical axis of the eye and the ultrasound beam is perpendicular to the retina, the retinal spike is displayed as a straight, steeply rising echo spike. When the probe is not properly aligned with the optical axis of the eye, the ultrasound beam is not perpendicular to the retinal surface and the retinal spike is displayed as a jagged, slow-rising echo spike. Repeated measurements are taken until a few equal measurements are obtained with sharp retinal spikes.
Ultrasound can be done with either contact or immersion methods. In the contact method, the probe touches the cornea and may result in corneal compression and a shorter AL. Corneal compression is more likely in pediatric eyes because of low corneal and sclera rigidity. Using the immersion technique, the ultrasound probe does not come into direct contact with the cornea, but instead uses a coupling fluid between the cornea and probe preventing corneal indentation. Immersion A-scan has been shown to be superior to contact biometry in children.11,12 If contact A-scan is used, it is important to make sure that the tip does not indent the cornea. Pediatric cataract surgeons use the contact technique more frequently when measuring the AL of pediatric eyes at the time of cataract surgery. This statement is based on 2009 e-mail survey sent to pediatric ophthalmologists, in which 173 (82.4%) surgeons reported using contact A-scan compared with
37 (17.6%) who reported using the immersion technique.12 Because of a lack of cooperation in the clinic setting, AL measurements in young children often must be obtained in the operating room under general anesthesia. In the operating room setting, an experienced ultrasonographer may not be available. Contact A-scan measurements are easier for the surgeon or an operating room technician to perform. Immersion A-scan requires more experience and practice and is best performed by an experienced ultrasonographer. In a prospective clinical trial, we compared AL measurements by contact and immersion techniques in pediatric cataractous eyes (n = 50 eyes of 50 children).12 AL was measured by both contact and immersion techniques for all eyes, randomized as to which to perform first to avoid measurement bias. AL measurement by contact technique was significantly shorter as compared with immersion technique (21.36 ± 3.04 mm and 21.63 ± 3.09 mm, respectively; P < 0.001). AL measurements using the contact technique were on an average 0.27 mm shorter than those obtained using the immersion technique. Forty-two eyes (84%) had shorter AL when measured using the contact technique as compared with the immersion technique. Lens thickness (LT) measurements by contact technique was not significantly different from that of immersion technique (3.61 ± 0.74 and 3.60 ± 0.67 mm, respectively; P = 0.673). Anterior chamber depth (ACD) measurements were significantly more shallow with the contact technique (3.39 ± 0.59 mm and 3.69 ± 0.54 mm, respectively; P < 0.001). As can be seen here, shorter AL in contact group was mainly as a result of ACD value rather than LT value. IOL power needed for emmetropia was significantly different (28.68 diopters [D] versus 27.63 D; P < 0.001). During IOL power calculation, if AL measured by contact technique is used, it will result in the use of an average 1-D stronger IOL power than is actually required. This can lead to induced myopia in the postoperative refraction. A consistent error could be compensated for by the addition of a constant or by formula personalization; however, this is not possible because the compression error varies from eye to eye.
37 (17.6%) who reported using the immersion technique.12 Because of a lack of cooperation in the clinic setting, AL measurements in young children often must be obtained in the operating room under general anesthesia. In the operating room setting, an experienced ultrasonographer may not be available. Contact A-scan measurements are easier for the surgeon or an operating room technician to perform. Immersion A-scan requires more experience and practice and is best performed by an experienced ultrasonographer. In a prospective clinical trial, we compared AL measurements by contact and immersion techniques in pediatric cataractous eyes (n = 50 eyes of 50 children).12 AL was measured by both contact and immersion techniques for all eyes, randomized as to which to perform first to avoid measurement bias. AL measurement by contact technique was significantly shorter as compared with immersion technique (21.36 ± 3.04 mm and 21.63 ± 3.09 mm, respectively; P < 0.001). AL measurements using the contact technique were on an average 0.27 mm shorter than those obtained using the immersion technique. Forty-two eyes (84%) had shorter AL when measured using the contact technique as compared with the immersion technique. Lens thickness (LT) measurements by contact technique was not significantly different from that of immersion technique (3.61 ± 0.74 and 3.60 ± 0.67 mm, respectively; P = 0.673). Anterior chamber depth (ACD) measurements were significantly more shallow with the contact technique (3.39 ± 0.59 mm and 3.69 ± 0.54 mm, respectively; P < 0.001). As can be seen here, shorter AL in contact group was mainly as a result of ACD value rather than LT value. IOL power needed for emmetropia was significantly different (28.68 diopters [D] versus 27.63 D; P < 0.001). During IOL power calculation, if AL measured by contact technique is used, it will result in the use of an average 1-D stronger IOL power than is actually required. This can lead to induced myopia in the postoperative refraction. A consistent error could be compensated for by the addition of a constant or by formula personalization; however, this is not possible because the compression error varies from eye to eye.
In a subsequent study, we compared prediction error (PE) and absolute prediction error (APE) using contact and immersion techniques.11 The contact and immersion A-scan biometry techniques had been performed in each eye and PE using each technique was compared. There was a significant difference in PE between contact and immersion A-scan biometry in children. The mean PE was +0.4 ± 0.7 D in the contact group and −0.4 ± 0.8 D in the immersion group (P < 0.001) and the mean APE was 0.7 ± 0.4 D and 0.7 ± 0.6 D, respectively (P = 0.694). The APE was <0.5 D in 5 eyes (23%) using the contact technique and in 11 eyes (50%) using the immersion technique. The mean postoperative spherical equivalent was +2.9 ± 2.5 D, which was significantly different from the mean predicted refraction for contact A-scan (3.3 ± 2.8 D; P = 0.010) but not immersion A-scan (2.5 ± 2.5 D; P = 0.065). Ben-Zion et al.13 compared PEs of 138 pediatric eyes measured by the contact A-scan technique with a later group of 65 children measured with the immersion technique. They found no significant difference in APE (1.11 and 1.03 D, respectively) and noted PE of +0.23 and −0.32 D with the contact technique and immersion technique, respectively.
Optical Biometry
Optical biometry is based on partial coherence interferometry (PCI)—IOLMaster (Carl Zeiss Meditec) or LenStar (Haag Strait). LenStar allows higher resolution compared with the IOLMaster. The measurement includes corneal thickness, ACD, LT, AL, keratometry, white-to-white distance, pupillometry, eccentricity of the visual axis, and retinal thickness at the point of fixation. It can also be used to access the horizontal iris width, pupil diameter, eccentricity of the visual axis, and retinal thickness. PCI has been used in cooperative children with reliability and accuracy. PCI requires patient cooperation and thus may not be a viable option in infants and young children. Claimed improvements over conventional ultrasound techniques include high reproducibility, contact-free measurements, and observer independence of the measurements. Lenhart et al.14 reported PE for AL measurements obtained using PCI versus immersion ultrasonography in children. AL measurements in the operative eye were obtained using PCI at the preoperative clinic visit and then using immersion US in the operating room before surgery. The data were compared to determine the degree of agreement. The charts of 18 patients (27 eyes) were reviewed. Preoperative AL measurements by PCI were obtained in 21 eyes (78%). On average, the PCI-measured ALs were 0.1 mm less than the immersion US values (95% confidence interval, −0.2 to −0.1; P = 0.002). All eyes with an AL of 23.5 mm or less had lower PCI values than immersion US values. There was no systematic pattern of 1 measurement being greater or lesser than the other in eyes with an AL longer than 23.5 mm. The authors concluded that there was a systematic difference in AL measurement between PCI and immersion technique, with PCI tending to give lower values, particularly in eyes with an AL of 23.5 mm or less. Gursoy et al.15 compared AL, ACD, and LT measured with LenStar with those obtained with A-scan contact technique. Right eyes of 565 school children were included (mean age 10.5 years). The mean difference between contact ultrasound and LenStar was −0.72, −0.27, and +0.24 mm for AL, ACD, and LT, respectively. PCI technology is not able to obtain measurements in eyes with dense cataract and in those that cannot fixate on the red light of the instrument because of inadequate vision. In children, the cataracts are often dense and fixation may be inadequate.
Biometry Values in Eyes with Pediatric Cataract
We reported biometry data of pediatric cataractous eyes (randomly selected single eye in bilateral cases; cataractous eye in unilateral cases).16 Three hundred ten eyes were analyzed, with a mean age at cataract surgery of 45.30 ± 48.1 months (median, 27.50; range, 0.23-203.08); mean AL of 20.52 ± 2.87 mm (range, 14.19-29.10); ACD of 3.29 ± 0.60 mm (range, 1.48-4.35); and LT of 3.62 ± 0.86 mm (range, 0.61-6.35). Table 5.1 shows the mean AL per age group. In Table 5.2, the first 2 years of life are divided into age groups, showing the mean AL per age group.
The overall mean AL of pediatric cataractous eyes (20.5 ± 2.9 mm) in our series was significantly different (P < 0.001) than the overall mean AL of pediatric non-cataractous eyes described in a Gordon and Donzis series (21.9 ± 1.6 mm).17 More important, the standard deviation was nearly two times more in eyes with cataract than in those without (±2.9 mm versus ±1.6 mm). This difference is a very important factor to keep in mind; that is, these cataractous eyes are abnormal to begin with, which may also lead to variations in postoperative growth. Eyes with cataract showed a shorter AL in the first 12 months of life (cataractous, 17.9 ± 2.0 mm; noncataractous, 19.2 ± 0.7 mm). In the first 12 months of life, the standard deviation was almost three times that of eyes without cataract (±2.0 mm versus ±0.7 mm).
Table 5.1 AL MEASUREMENTS IN UNILATERAL AND RANDOMLY SELECTED SINGLE EYES OF PEDIATRIC PATIENTS WITH BILATERAL CATARACTS, CATEGORIZED BY AGE | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|



