Hemostasis is essential during endoscopic sinus and skull base surgery. Patients must be adequately assessed for bleeding risk to appropriately consent to surgery. The patient and the surgeon must be aware of the individual bleeding risk for a given procedure. A thorough history and physical examination is the best screening methodology available to determine whether a patient requires further hematologic work-up. Included in this assessment should be any medications and herbals that the patient consumes. This ensures a safe evaluation of the patient, streamlines appropriate consultation and testing when necessary, and confers accurate surgical risk assessment.
Key learning points
At the end of this article, the reader will:
- •
Be able to identify patients who are in the high-risk category for bleeding during surgery.
- •
Be able to ask relevant questions to delineate a significant history of hemostatic deficits.
- •
Be able to recognize the common coagulation disorders.
- •
Be familiar with pertinent anticoagulant medications and their perioperative management.
- •
Be familiar with herbal medicines that confer bleeding risk.
- •
Be able to describe diagnostic tests for coagulation disorders.
- •
Be able to determine when a referral to a hematologist is required.
Introduction
Hemostasis is essential during endoscopic sinus and skull base surgery. Patients must be adequately assessed for bleeding risk to appropriately consent to surgery. The patient and the surgeon must be aware of the individual bleeding risk for a given procedure. A thorough history and physical examination is the best screening methodology available to determine whether a patient requires further hematologic work-up. Included in this assessment should be any medications and herbals that the patient consumes. This ensures a safe evaluation of the patient, streamlines appropriate consultation and testing when necessary, and confers accurate surgical risk assessment.
Introduction
Hemostasis is essential during endoscopic sinus and skull base surgery. Patients must be adequately assessed for bleeding risk to appropriately consent to surgery. The patient and the surgeon must be aware of the individual bleeding risk for a given procedure. A thorough history and physical examination is the best screening methodology available to determine whether a patient requires further hematologic work-up. Included in this assessment should be any medications and herbals that the patient consumes. This ensures a safe evaluation of the patient, streamlines appropriate consultation and testing when necessary, and confers accurate surgical risk assessment.
Discussion
- •
Hereditary bleeding tendency
- •
Personal or family history of predisposition to bleeding
- •
Abnormal coagulation testing results
- •
Coexisting medical conditions
- •
Medication use (including herbal)
- •
Need for antithrombotic therapy in the perioperative period
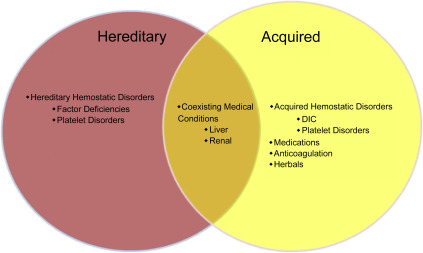
Patients at risk for bleeding during the perioperative period include those with a hereditary disorder, especially with a suggestive family history. Abnormal coagulation results can sometimes indicate an underlying hemostatic disorder, but the prevalence of inherited coagulopathies is low. Furthermore, some patients with inherited coagulopathies require specific testing to diagnose and have normal results on routine screening with prothrombin time, international normalized ratio, and partial thromboplastin time. Concomitant medical conditions, such as hepatic or renal dysfunction, medications, and herbal medications, significantly influence a patient’s hemostatic tendencies. It is pertinent to determine whether patients are at increased bleeding risk before surgery to obtain the best possible outcomes ( Fig. 1 ).
- •
Adequate history
- •
Important to diagnose because
- ○
Appropriate precautions can be taken
- ○
Risk assessment can be outlined to patient
- ○
If hereditary disorder found, other family members can be screened (ie, hemophilia A)
- ○
The most effective means of screening patients for potential surgical hemorrhage is an adequate and thorough patient history. Laboratory testing should not be used in lieu of a patient history because inconclusive testing results are common. The importance of diagnosing a hereditary bleeding disorder is of obvious importance for the patient, but also has potential impact on family members in the future.
- •
Most common
- ○
Hemophilia A (factor VIII deficiency)
- ○
Hemophilia B (factor IX deficiency)
- ○
von Willebrand disorder (vWD)
- ▪
Mild (prevalence is 0.8%–1.6% )
- ▪
Overall prevalence is 1%
- ▪
- ○
- •
Less common
- ○
Factor I
- ○
Factor II
- ○
Factor V
- ○
Factor X
- ○
Factor XI
- ○
Factor XII
- ○
Platelet disorders
- ○
- •
Rare
- ○
α 2 -Antiplasmin deficiency
- ○
α 1 -Antitrypsin Pittsburgh deficiency
- ○
Combined factor deficiencies
- ○
Notable and common factor/hereditary bleeding disorders include hemophilia A and B and vWD. Hemophilia A stems from a deficiency of factor VIII, which itself is activated by thrombin to become a cofactor for the synthesis of activated factor Xa, a major mediator of the common pathway. Hemophilia B is explained by a deficiency in factor IX, the activated form of which is also a cofactor in the production of activated factor Xa. vWD is the most prevalent coagulation disorder, where there is a deficiency in von Willebrand factor (vWF). vWF is important in platelet adhesion to the subendothelium and binding factor VIII. Consequently, the half-life of factor VIII is significantly shortened without vWF.
The extremely rare disorders listed have all been case reports with approximately 50 cases/families reported for all three deficiencies. Fig. 2 shows the coagulation cascade with appropriate markings highlighting the physiology of hemophilia A, hemophilia B, and vWD.
- •
Unreliable historian: patient does not recognize bleeding disorder
- •
Patient not exposed to significant bleeding risk, such as trauma, surgery, or dental extractions (ie, factor XI deficiency)
- •
Acquired hemostatic defects (ie, thrombocytopenia)

Laboratory tests for hemostasis are advisable if patients are undergoing high-risk surgery, even when adequate history is obtained that does not suggest a bleeding problem. A patient at risk for perioperative bleeding could still be detected on the basis of laboratory screening tests because the patient may not yet have been exposed to surgical tests of hemostasis, such as dental extractions and trauma. In fact, factor XI deficiency results in significant bleeding only after major trauma or surgery. Furthermore, the patient could have acquired a hemostatic defect later in life that has been asymptomatic up until the point of consult.
- •
Have you ever bled for a long time? Specifically, have you had profuse menstrual bleeding, blood in the stool, or bleeding into a muscle or a joint?
- •
Have you had either immediate or delayed significant bleeding following a dental extraction?
- •
Do any of your immediate family members have a problem with unusual bruising or bleeding after surgery?
- •
Do you bruise without an inciting event?
- •
What operations/procedures have you undergone (including minor procedures, such as biopsies or endoscopies)? Have you ever developed significant bleeding or bruising afterward? Did you require blood transfusions?
- •
What pain medications do you take? Do you take over-the-counter supplements or herbal remedies?
This is a concise list of questions to screen patients for potential hemostatic bleeding disorders. This aims to be a supplement to a full interview consisting of past medical history, past surgical history, medications, and allergies. Asking specifically about patients and family members’ reactions to surgery and dental extractions may help elucidate abnormal bleeding that the patient themselves does not recognize. Asking about bruising without an inciting event may help to identify patients with an acquired disorder or one that was previously undiagnosed. From the answers to these questions the surgeon can develop levels of increasing concern for surgical hemostatic risk and several risk categories have been described in the past. A proposed stratification of surgical hemostatic risk is shown in Table 1 .
- •
Petechiae
- •
Ecchymosis
- •
Telangiectasias
- •
Stigmata of prior hemarthroses (joint deformities)
- •
Hematomas
- •
Stigmata of Ehlers-Danlos syndrome: skin hyperelasticity and hyperextendable joints
- •
Stigmata of vitamin C deficiency: bleeding gums, poor wound healing
- •
Stigmata of Cushing syndrome: skin atrophy, striae, hyperpigmentation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


