Purpose
To document changes in metamorphopsia via preferential hyperacuity perimeter and to identify prognostic factors related to favorable metamorphopsia outcome after idiopathic epiretinal membrane surgery.
Design
Prospective, consecutive, interventional case series.
Methods
We prospectively included 29 eyes of 27 patients who underwent successful vitrectomy for idiopathic epiretinal membrane. All eyes underwent examinations before surgery and at 2 weeks and 1, 3, and 6 months after surgery. Metamorphopsia was assessed by using a preferential hyperacuity perimeter. Several clinical factors were analyzed to reveal relationships with final metamorphopsia outcome, including the duration of symptoms, best-corrected visual acuity, and spectral-domain optical coherence tomography findings. Spectral-domain optical coherence tomography findings included assessment of central foveal thickness, and the integrity of the photoreceptor inner segment and outer segment (IS/OS) junction.
Results
At baseline, preferential hyperacuity perimeter detected areas of distortion in 15 eyes (51.7%). At 6 months after surgery, there was significant reduction in metamorphopsia ( P = .001), which was paralleled with significant improvement of best-corrected visual acuity and reduction of central foveal thickness ( P < .001). At 6 months after surgery, the degree of metamorphopsia was related significantly to the severity of preoperative metamorphopsia and central foveal thickness at baseline (ρ = 0.856; P < .001; ρ = 0.412; P = .027; respectively). Eyes with broadly disrupted IS/OS junction of more than 200 μm before surgery revealed significantly poorer postoperative metamorphopsia than those with intact or narrowly disrupted IS/OS junction ( P = .001). However, duration of symptoms and baseline best-corrected visual acuity were not correlated with final metamorphopsia ( P = .625 and P = .052, respectively).
Conclusions
Significant reduction of metamorphopsia paralleled the improvement of best-corrected visual acuity and central foveal thickness until 6 months after idiopathic epiretinal membrane surgery. The significant predictors for postoperative metamorphopsia outcome were the degree of preoperative metamorphopsia, central foveal thickness, and the photoreceptor IS/OS junction integrity at baseline.
Idiopathic epiretinal membrane (ERM) is a macular pathologic feature characterized by fibrocellular proliferation on the internal limiting membrane of the macula. In early-stage ERM, there are no symptoms, whereas advanced ERM causes various visual impairments. Metamorphopsia is an important visual symptom of ERM and may affect a patient’s daily life. Even after successful ERM surgery leading to a significant improvement in visual acuity, residual metamorphopsia may affect patients’ vision-related quality of life. In most studies, evaluation of functional outcomes after vitrectomy with ERM peeling has been limited to assessing visual acuity; such studies have not evaluated the influence of surgery on metamorphopsia properly.
However, there are methods that may be used to evaluate metamorphopsia in eyes with ERM, including assessments based on the use of Amsler charts, M-CHARTS (Inami Co, Tokyo, Japan), binocular correspondence perimetry, and preferential hyperacuity perimeter. Preferential hyperacuity perimeter is a macular perimeter that is based on the visual function of hyperacuity, which is the ability to perceive a difference between the relative spatial localization of 2 or more visual stimuli. Preferential hyperacuity perimeter was developed originally to monitor the progression to neovascular age-related macular degeneration by detecting the severity of visual defects, such as metamorphopsia and scotoma. However, a main cause of metamorphopsia is photoreceptor or outer segment disarray resulting from the contraction of epiretinal membranes in patients with ERM. Preferential hyperacuity perimeter identifies such disarrangement of photoreceptors as distortion, scotoma, or blurring. Although preferential hyperacuity perimeter may be influenced by the localized spatial discrimination ability of the subject and the motor function of the observer, its usefulness for the detection and quantification of metamorphopsia in eyes with ERM has been reported.
The purpose of this study was to document changes in metamorphopsia via preferential hyperacuity perimeter and to identify prognostic factors related to a favorable metamorphopsia outcome after idiopathic ERM surgery.
Methods
This prospective, consecutive, interventional case series included patients who underwent a standard 23-gauge vitrectomy for idiopathic ERM by 1 retinal surgeon (H.K). Surgery was conducted in patients with a reduction of visual acuity of less than 20/40 or in those who reported visual disturbances such as metamorphopsia. If a decreasing trend in visual acuity was associated with an increasing trend of retinal thickness of more than 350 μm or with disruption of the photoreceptor inner segment and outer segment (IS/OS) junction before surgery, surgery was performed. The exclusion criteria were: (1) secondary ERM including diabetic retinopathy, venous occlusion, retinal detachment, age-related macular degeneration, uveitis, or trauma; (2) macular or lamellar hole; (3) previous vitreoretinal surgery; (4) myopia with less than −6.0 diopters (D) or a 26-mm greater axial length; (5) other ocular pathologic features that could interfere with visual outcome; (6) opaque optical media that significantly affects vision or disturbs optical coherence tomography (OCT) image acquisition, including cataract of more than Emery-Little classification grade 3; and (7) significant postvitrectomy complications that interfere with visual outcome and require surgical intervention.
All patients underwent a standard 3-port, 23-gauge pars plana vitrectomy using the Associate vitrectomy unit (Dutch Ophthalmic Research Center, Zuidland, The Netherlands). After displacement of the conjunctiva, oblique-angled sclerotomies were made by using a 2-step cannula system perpendicular to the limbus. The posterior hyaloid membrane was detached using an ocutome, if a posterior vitreous detachment was not present. The ERM peeling was conducted using end-gripping forceps (Alcon Surgical, Fort Worth, Texas, USA) with the assistance of triamcinolone acetonide. In 3 (10.3%) of the 29 eyes, subsequent peeling of the internal limiting membrane was carried out at the surgeon’s discretion, without staining. If a clinically significant cataract was present, phacoemulsification with intraocular lens implantation was performed during vitrectomy.
All patients underwent full ophthalmologic examinations before surgery and at 2 weeks and 1, 3, and 6 months after ERM removal. Examinations included measurement of best-corrected visual acuity (BCVA) and intraocular pressure, along with anterior segment evaluation by slit lamp, dilated fundus examination, spectral-domain (SD) OCT (Cirrus; Carl Zeiss Meditec AG, Jena, Germany), and preferential hyperacuity perimeter (PreView PHP; Carl Zeiss Meditec AG). BCVA was measured by using a Snellen chart, with the results converted to the logarithm of the minimal angle of resolution scale. Central foveal thickness was measured by using SD OCT in Macular Cube 512 × 128 mode, covering a retinal area of 6.0 × 6.0 mm. The profile of the photoreceptor layer was evaluated on horizontal and vertical cross-sectional SD OCT macular images obtained by using the 5-line raster scan mode; gray-scale images were used to increase identification precision. The profile of the photoreceptor IS/OS junction was the hyper-reflective layer above the retinal pigment epithelium. The photoreceptor layer status within 500 μm in either direction of the fovea was evaluated independently by 2 of the authors (S.B. and W.N.), after which consensus was derived. The integrity of the photoreceptor IS/OS junction was graded from 0 to 2: grade 0 indicated a continuous photoreceptor IS/OS junction, grade 1 indicated the presence of an irregularity or a focal disruption of 200 μm or less, and grade 2 indicated the presence of a broad disruption more than 200 μm.
Metamorphopsia assessment was performed by using the preferential hyperacuity perimeter, as described by the developers. The examination distance was 50 cm, and the patient’s distance refraction was adjusted to a near distance of 50 cm. The dotted lines with slight misalignment of a few dots stimulus was applied to the central 14 degrees of retina with a spatial resolution of 0.75 degrees. To cover the entire visual field, a series of stimuli were flashed on various locations in a random order. When the degree of misalignment exceeds a threshold value, the patient may perceive an artificial distortion. In such a case, the patient was instructed to touch the location of the abnormal perception on the instrument’s screen. However, if the stimulus is presented on a pathologic retina, the patient may perceive pathologic distortion, scotoma, or blurring. In the perception competition between artificial and pathologic distortions, the brain ignores the smaller stimuli. Based on the difference in magnitude between artificial and pathologic distortions, preferential hyperacuity perimeter can quantify the patient’s degree of pathologic distortion. By using the developers’ algorithm, the magnitude of the visual field defect is determined and displayed on a 2-dimensional map of visual field. In addition, the preferential hyperacuity perimeter provides estimates of several quantitative parameters that indicate the size and severity of metamorphopsia and that can be compared with values in a normal database. Those parameters include: areas of different severity level, peak score values, and total volume. In this study, the sum of preferential hyperacuity perimeter-derived total volume was used to assess the changes in metamorphopsia.
Statistical analyses were performed using SPSS version 17.0 (SPSS Inc, Chicago, Illinois, USA). All comparisons were 2-tailed. The comparisons between the preoperative and postoperative values were evaluated using the Wilcoxon signed-rank test. The Spearman rank correlation test was used to analyze the relationships between BCVA, central foveal thickness, and total volume. Comparisons between 2 groups were conducted using the Mann–Whitney U test. An analysis of variance was performed to determine the significance of differences in total volume when associated with the grades of photoreceptor IS/OS junction integrity. That analysis was followed by Bonferroni post hoc testing for multiple comparisons. The statistical significance level was set at P < .05.
Results
Twenty-nine eyes of 27 patients who underwent vitrectomy for idiopathic ERM were included in this study. The subjects included 8 men (9 eyes; 31.0%) and 19 women (20 eyes; 69.0%). The mean age of the patients was 64.2 ± 6.6 years (range, 45 to 76 years). The mean duration of symptoms was 17.1 ± 15.2 months (range, 1 month to 6 years). Twenty-three eyes (79.0%) were phakic and 6 eyes (21.0%) were pseudophakic at baseline (before vitrectomy). Concomitant cataract surgery was performed in 19 of the eyes undergoing ERM peeling. Among 23 phakic eyes at baseline, 4 eyes (17.4%) remained phakic after surgery, and those did not exhibit cataract progression within the 6 months after surgery.
Functional and Anatomic Changes After Epiretinal Membrane Peeling
The mean logarithm of the minimal angle of resolution BCVA at baseline was 0.4 ± 0.2 (range, 0.1 to 0.82). After ERM peeling, the mean BCVA improved significantly at each follow-up period compared with that at baseline ( P < .001; Table 1 ). The final mean BCVA value of 0.1 ± 0.1 was achieved at 6 months after surgery. At 1 month after surgery, 71.5% of the total increase in BCVA was obtained.
| Time Point | Best-Corrected Visual Acuity (logMAR) | Central Foveal Thickness (μm) | Total Volume a |
|---|---|---|---|
| Baseline | 0.4 ± 0.2 | 435.6 ± 86.3 | 5100.2 ± 12141.9 (9860.5 ± 15638.5) |
| 2 wks | 0.3 ± 0.2 b | 376.2 ± 69.7 b | 4179.3 ± 7339.1 (8080.1 ± 8599.7) |
| 1 mo | 0.2 ± 0.1 b | 377.0 ± 108.3 b | 2739.1 ± 4375.7 (5295.5 ± 4877.3) |
| 3 mos | 0.1 ± 0.1 b | 349.3 ± 77.9 b | 2156.4 ± 4581.4 b (4169.0 ± 5743.6 b ) |
| 6 mos | 0.1 ± 0.1 b | 340.0 ± 68.7 b | 1378.0 ± 2544.3 b (2664.2 ± 3045.6 b ) |
a A preferential hyperacuity perimeter parameter representing metamorphopsia (arbitrary units). Values in brackets are the mean total volumes of 15 eyes that exhibited preoperative metamorphopsia.
b Significant difference ( P < .05) from baseline value of each parameter.
The mean central foveal thickness at baseline was 435.6 ± 86.3 μm (range, 276 to 610 μm). After ERM peeling, the mean central foveal thickness decreased significantly at each follow-up compared with the thickness at baseline ( P < .001; Table 1 ). The final central foveal thickness of 340.0 ± 68.7 μm was obtained at 6 months after surgery. Within 1 month after surgery, 61.3% of the total reduction in central foveal thickness was achieved.
The grading of photoreceptor IS/OS junction integrity at baseline was: grade 0 (continuous photoreceptor layer) in 12 eyes (41.4%), grade 1 (irregularity or small disruption) in 13 eyes (44.8%), and grade 2 (broad disruption) in 4 eyes (13.8%). At 6 months after surgery, the photoreceptor IS/OS junction grading was: grade 0 in 14 eyes (48.3%), grade 1 in 10 eyes (34.5%), and grade 2 in 5 eyes (17.2%), a grading distribution that was not significantly different from that at baseline ( P = .72). Complete restoration of the photoreceptor IS/OS junction was observed in 3 eyes (10.3%) at 6 months after surgery; each of those eyes had grade 1 IS/OS junction integrity at baseline. However, disruption of IS/OS junction integrity was greater in 2 eyes (6.9%) at 6 months after surgery: 1 eye degenerating from grade 1 to grade 2 and 1 eye from grade 0 to grade 1.
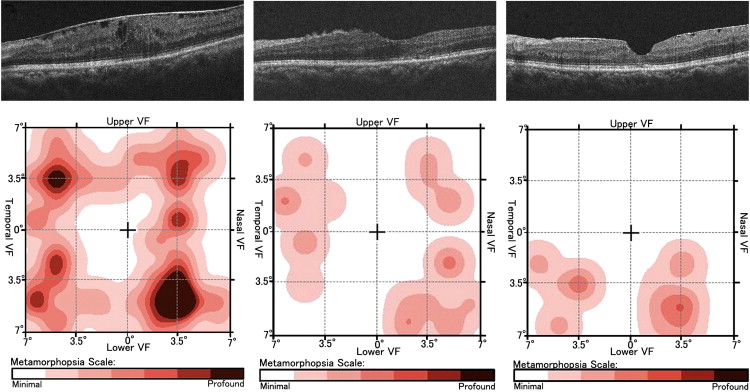
At baseline, the preferential hyperacuity perimeter detected areas of distortion in 15 eyes (51.7%), whereas 14 eyes (48.5%) did not exhibit any abnormalities. In the 15 eyes with metamorphopsia at baseline, the mean total volume was 9860.5 ± 15 638.5 (range, 1058 to 63 534; Table 1 ). After surgery, the mean total volume gradually decreased from the baseline, but the reduction in total volume did not show statistical significance until 3 months after surgery. At 6 months after surgery, the mean total volume of the 15 eyes with preoperative metamorphopsia was 2664.2 ± 3045.6, and complete regression of metamorphopsia was achieved in 5 eyes (33.3%). At 1 month after surgery, there was a 63.4% reduction in mean total volume of 15 eyes with preoperative metamorphopsia.
In contrast, in all eyes without metamorphopsia at baseline, there were no preferential hyperacuity perimeter abnormalities detected at any of the follow-up times after ERM peeling. Figure 1 shows the changes in each clinical parameter in 1 patient with idiopathic ERM before and after surgery.
Relationships Between Clinical Parameters and Preoperative Metamorphopsia
There were no significant differences in baseline clinical parameters between the groups with and without baseline metamorphopsia, including age, sex, duration of symptoms, BCVA, and IS/OS junction integrity ( Table 2 ). However, the preferential hyperacuity perimeter indicated that the mean central foveal thickness at baseline was significantly greater in eyes with preoperative metamorphopsia (468.3 ± 81.7 μm) than in those without baseline metamorphopsia (400.6 ± 79.5 μm; P = .047).
| Baseline Parameter | Preoperative Metamorphopsia (n = 15) | No Preoperative Metamorphopsia (n = 14) | P Value |
|---|---|---|---|
| Age (y) | 65.7 ± 6.1 | 60.5 ± 7.7 | .057 |
| Sex (male:female) | 5:10 | 4:10 | 1.0 |
| Duration of symptoms (mos) | 19.3 ± 17.3 | 14.7 ± 12.9 | .355 |
| Metamorphopsia (total volume a ) | 9860.5 ± 15638.5 | 0 | <.001 |
| Best-corrected visual acuity (logMAR) | 0.5 ± 0.2 | 0.3 ± 0.2 | .054 |
| Central foveal thickness (μm) | 468.3 ± 81.7 | 400.6 ± 79.5 | .047 |
| Integrity of photoreceptor layer, b no. of eyes (%) | |||
| Grade 0 | 5 (33.3) | 8 (35.7) | .097 |
| Grade 1 | 6 (40.0) | 6 (50.0) | |
| Grade 2 | 4 (26.7) | 0 (14.3) |
a A preferential hyperacuity perimeter parameter representing metamorphopsia (arbitrary units).
b The integrity of the photoreceptor inner segment/outer segment (IS/OS) junction was graded from 0 to 2: grade 0 indicated a continuous photoreceptor IS/OS junction, grade 1 indicated presence of irregularity or a focal disruption of 200 μm or less, and grade 2 indicated broad disruption of more than 200 μm.
Relationships Between Clinical Parameters and Final Metamorphopsia Outcome
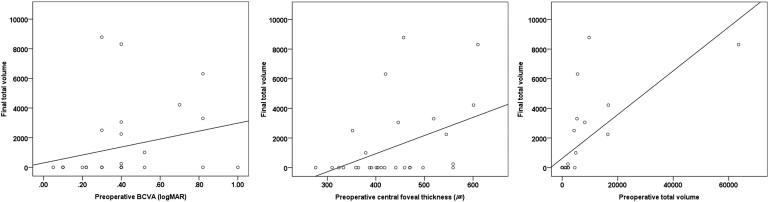
Baseline values of each clinical parameter for the 29 study eyes were analyzed to reveal relationships with final metamorphopsia outcome as measured by using preferential hyperacuity perimeter-derived total volume ( Figure 2 ). The final total volume was related significantly with preoperative total volume, as well as with central foveal thickness and IS/OS junction grade at baseline (ρ = 0.856; P < .001; ρ = 0.412; P = .027; P = .001; respectively). The mean total volume in eyes with broadly disrupted IS/OS junctions (grade 2) was significantly greater than that in IS/OS junction grade 0 or grade 1 eyes ( P < .01, Bonferroni test; Table 3 ). In contrast, duration of symptoms and BCVA at baseline were not correlated with the final total volume (ρ = 0.095; P = .625; ρ = 0.365; P = .052; respectively).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


