Testing category
Specific test(s)
Tests for a general clinic
Tests for a specialized unit
Symptoms
Questionnaires
McMonnies, Schein, OSDI, DEQ, OCI, SPEED, and others
McMonnies, Schein, OSDI, DEQ, OCI, SPEED, and others
Signs
Meibomian function
Lid morphology
Slit lamp microscopy
Slit lamp microscopy, confocal microscopy
Meibomian gland mass
Slit lamp microscopy
Meibography
Gland expressibility, expressed oil quality and volume
Interferometry, slit lamp
Slit lamp microscopy
Lid margin reservoir
Tear film lipid layer, thickness, spread time, spread rate
Evaporation tears
Evaporimetry
Evaporimetry
Osmolarity
Osmolarity
TearLab device, others
TearLab device, others
Stability
Tear film
TFBUT, ocular protection index
TFBUT, ocular protection index
Tear film lipid layer
Spread time
Interferometry, spread rate, pattern
Indices of volume and secretion
Tear secretion
Schirmer 1
Fluorophotometry/fluorescein clearance rate
Tear volume
Not available
Volume by fluorophotometry
Tear volume
Meniscus height
Meniscus radius of curvature, meniscometry
Tear clearance
Tear film index
Tear film index
Ocular surface
Ocular surface staining
Oxford scheme; NEI/industry scheme
Oxford scheme, NEI/industry scheme
Inflammation
Biomarkers
Flow cytometry, bead arrays, microarrays, mass spectrometry, cytokines and other mediators, interleukins, matrix metalloproteinases
A practical approach to diagnosis needs to be more abbreviated and selective. The order that tests are performed is also important. The performance of one test needs to ideally not affect the result of the next.
For example, Schirmer testing will cause significant irritation and inferior punctate epithelial erosions. This obviously will affect the examination findings with fluorescein.
My suggested order of tests would be (Nichols et al. 2011):
1.
Symptom questionnaire
2.
Clinical history
3.
Tear film break-up time (TFBUT) with fluorescein
4.
Corneal staining with fluorescein
5.
Schirmer 1
6.
Lid margin examination
7.
Meibomian gland expression
3.1 Focusing Your Diagnostic Testing
The focus of your diagnostic testing should be to identify a few key questions necessary to guide management.
Key Questions Are
1.
What are key symptoms of dry eye experienced?
2.
What is the severity of the dry eye?
3.
Is this evaporative tear loss (meibomian gland dysfunction) or is this aqueous deficiency (Sjogren’s syndrome)?
4.
Is there any underlying cause that needs additional treatment and investigation?
Table 3.2 summarizes current diagnostic methods that can achieve this effectively and efficiently.
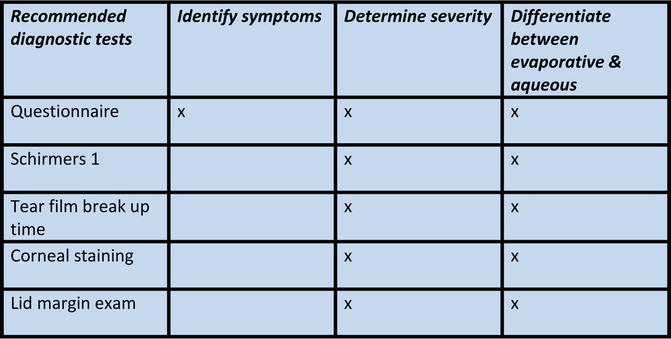
Table 3.2
Current diagnostic methods
3.2 Answering the Key Questions
3.2.1 Key Question 1: Identify and Rank Key Symptoms
Use a validated dry eye questionnaire such as the OSDI (Ocular Surface Disease Index Table 3.3) (Schiffman et al. 2000).
Table 3.3
Image courtesy of Allergan, Inc
Use your own personal standard modified questionnaire with severity scores so that an objective rating can be generated. For an example, see Table 3.4.
Table 3.4
Dry eye questionnaire
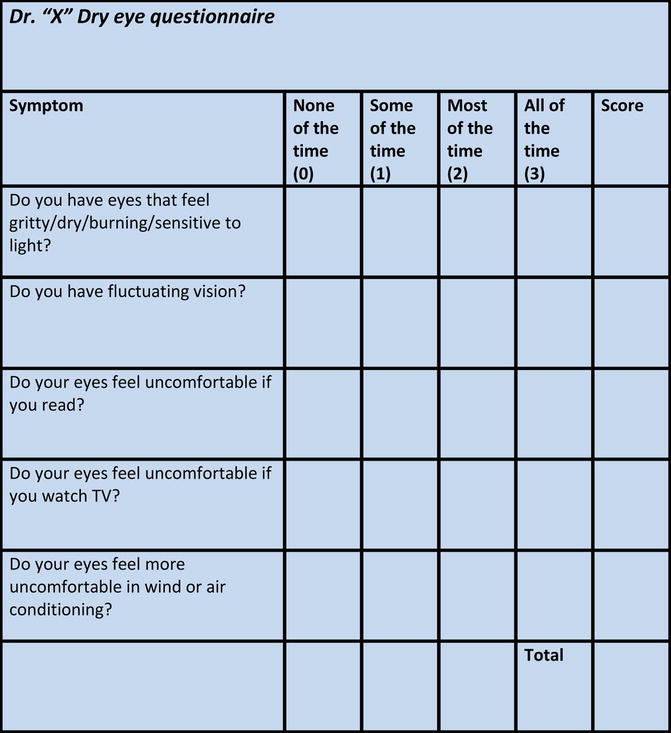
This can be easily filled out by the patient in the waiting room and saves your time during the consultation.
Allows you to monitor objectively the success of treatment.
3.2.2 Key Question 2: Determine the Severity of Dry Eye
The questionnaire (as above) will allow you to gauge severity based on symptoms.
The three signs recommended and traditionally used are:
A.
Schirmer 1, i.e., Schirmer without anesthetic
B.
Tear film break-up time (TFBUT) with fluorescein
C.
Corneal staining with fluorescein
3.2.2.1 Tips
A.
Schirmer 1.
Schirmer 1 tends to be more useful if positive, i.e., less than 10 mm of strip wetting. Scores of above 10 show less repeatability. Therefore, a Schirmer appears to be more useful in advanced disease (Nichols et al. 2004).
I typically do the Schirmer 1 test at the initial consultation to determine the severity of the dry eye and whether aqueous dysfunction exists but find it an unreliable method for monitoring treatment success. TFBUT seems to be a better method of monitoring treatment success.
Performance of Schirmer test (Kaštelan et al. 2013; DEWS 2007):
Place the Schirmer strip between the junction of the middle and outer third of the lower lid (Fig. 3.1).

Fig. 3.1
Place the Schirmer strip between the junction of the middle and outer third of the lower lid
Ask the patient to close their eyes.
Note the time.
Remove the strips after 5 min, or until the strips are completely saturated with tears, if sooner.
B.
TFBUT.
TFBUT values can differ greatly depending on method of fluorescein instillation, i.e., type and concentration of fluorescein used and time elapsed since fluorescein instilled.
TFBUT was found to become sensitive and specific as an indicator of dry eye than tear osmolarity the more severe the dry eye is (Lemp et al. 2011).
Apply one drop of 0.5 % fluorescein dye to the conjunctival fornix of each eye.
Ask patient to blink strongly to squeeze out the excess dye.
Wait 2 min for the fluorescein to diffuse and stain the pre-corneal tear film and tear meniscus.
Ask the patient to blink once and hold their eyes open.
The TFBUT is the number of seconds between the patient’s last blink and the first appearance of a random dry spot on the cornea (Fig. 3.2).
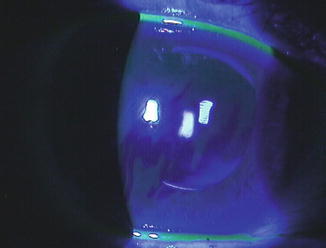
Fig. 3.2
The TFBUT is the number of seconds between the patient’s last blink and the first appearance of a random dry spot on the cornea
Three consecutive readings should be taken for each eye and the mean value recorded.
C.
Corneal staining with fluorescein.
The presence of any corneal staining according to the DEWS classification indicates already moderate to severe dry eye. Therefore, any corneal staining should be a red flag even if the patient is minimally symptomatic.
Performance of corneal staining (Kaštelan et al. 2013; DEWS 2007):
Perform steps outlined for TFBUT.
Note and count punctate epithelial erosions/PEE (Fig. 3.3).
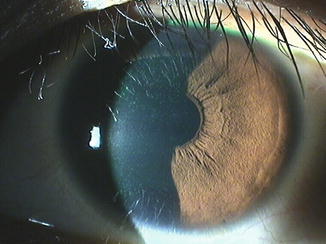
Fig. 3.3
Note and count punctate epithelial erosions/PEE
If 1–5 PEE are seen, the corneal score is 1; if 6–30 PEE are seen, the score is 2; if >30 PEE are seen, the score is 3.
Add another point up to a maximum of 6:
If PEE occur in the visual axis (central 3 mm of the cornea)
If one or more patches of confluent staining are seen anywhere on the cornea
If one or more corneal filaments are seen anywhere on the cornea
3.2.3 Key Question 3: Differentiate Between Meibomian Gland Dysfunction/MGD (Evaporative) and Sjogren’s (Aqueous) (Tong et al. 2010)
Remember MGD accounts for the vast majority of dry.
Dry eye symptoms that get worse with wind/air conditioning are more indicative of an evaporative issue.
Which of the two signs (Schirmer versus TFBUT) is lower will indicate which is the more likely cause. In severe dry eye states, both signs will have low scores as primary aqueous deficiency will cause secondary meibomian gland dysfunction and vice versa.
Serology testing and questioning about associated dry mouth/joint issues may help diagnose Sjogren’s though serology has a high false-negative rate (about 20 %). It is worthwhile retesting for Sjogren’s after a few years as patients can become seropositive. Consider a salivary gland biopsy if serology is negative and you or the patient want to pursue a definitive diagnosis (Qin et al. 2013).
D.




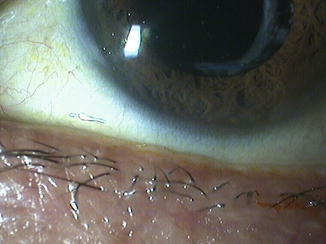
Examination of the lid margin.
The upper and lower lid margin should be examined closely for the following signs:
Blepharitis/scale
Expressibility (Table 3.5)
Table 3.5
Clinical summary of the MGD staging used to guide treatment
Stage
MGD grade
Symptoms
Corneal staining
1
+ (minimally altered expressibility and secretion quality)
None
None
2
++ (mildly altered expressibility and secretion quality)
Minimal to mild
None to limited
3
+++ (moderately altered expressibility and secretion quality)
Moderate
Mild to moderate; mainly peripheral
4
++++ (severely altered expressibility and secretion quality)
Marked
Marked; central in addition
“Plus” disease
Coexisting or accompanying disorders of the ocular surface and/or eyelids
Vascularization
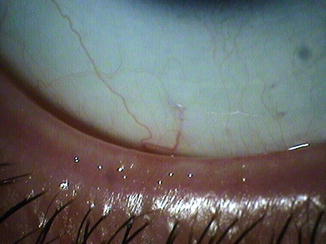
Vascularization and lid notching are signs of severe and chronic MGD. Vascularization may be more pronounced in ocular rosacea. Lid notching indicates meibomian gland atrophy, which is the end result of chronic MGD.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
