12 Powered Instrumentation in Endoscopic Sinus Surgery Throughout history, technological innovations have both facilitated and advanced the practice of endoscopic sinus surgery (ESS). The development of the Hopkins rod provided a high-clarity view of sinonasal anatomy and facilitated the first attempts at endoscopic surgery of the sinuses.1 With the introduction of the Hopkins rod, one of the surgeon’s hands was occupied at all times holding the scope, which means the surgeon needed to change instruments frequently with the remaining hand. This proved cumbersome at times, and predictably led to the development of multifunctional tools that would streamline surgery. This ushered in the era of powered instrumentation for ESS. As the field of rhinology advanced, surgeons were able to safely venture beyond the confines of the nose and paranasal sinuses to the orbit, skull base, and even into the intracranial cavity. As surgeons push the envelope of endoscopic surgery, they encounter new obstacles, such as the need to safely remove thick bone. New surgical obstacles often become the impetus for technological innovations. In this chapter, we have chosen to focus on technologies that we believe have had, or will have, the greatest impact on the field of ESS: the microdebrider, suction–irrigation drill, radiofrequency ablation, and ultrasonic aspirator.2–4 This chapter will succinctly outline the basic science of each of these technologies and summarize the available literature on indications for use, safety, and efficacy. We hope to highlight any controversies in the literature, and provide a critical review of the technologies that will allow the reader to determine what role, if any, these technologies may have in the scope of their practice. Defined as an electrically powered, cylindrical shaver that uses continuous suction for tissue removal,5 the microdebrider was first described in the medical literature by the House group as an instrument to morselize acoustic neuromas.4 It also became a popular tool among orthopedic surgeons as it was used in arthroscopic surgery. Setliff, Goode, and Parsons all published articles describing the use of the microdebrider in ESS for the first time in 1996.6–8 Since its initial foray into rhinology, there have been many articles published on the use of microdebrider in ESS. The ability of the microdebrider to continuously suction blood away from the surgical field while removing tissue and thin bone have made it the most popular powered instrument used by modern rhinologists. For this reason, many herald microdebrider as one of the most significant technological advances in the field of rhinology.5 There are several companies that manufacture microdebriders for ESS including Olympus-Gyrus (Gyrus, Bartlett, Tennessee, United States), Medtronic-Xomed (Medtronic, Jacksonville, Florida, United States) and Stryker (Stryker Corporation, Kalamazoo, Michigan, United States). Each company offers a product with unique design differences, but all microdebriders consist of a hollow shaft with a rotating, or oscillating, blade within the inner cannula. Continuous suction applied to the inner cannula draws soft tissue and bone chips into the blade. The tissue is cleaved by the oscillation of the blade and suctioned away from the operative field toward the suction canister, where it may be captured in a filter. Importantly, studies have shown that the tissue within the filter is histologically preserved for pathological examination.5 Some models have a serrated edge on the blade, which allows for better gripping of soft tissue and more aggressive tissue take down. In contrast, straight edges are considered less traumatic and more sparing of adjacent mucosal tissues. Blades can be set to continuously rotate (forward or backward) or oscillate (back and forth across the aperture). For soft tissue removal, the oscillation mode is used at slower speeds of 3000 to 5000 revolutions per minute (RPM) allowing the blade to stay open longer, and more soft tissue to be drawn into the aperture before it is cut. There are also specialized solid burr-like tips available for the microdebrider that allow a drilling action. These tips are beneficial when the surgeon encounters bone that is thicker than the conventional microdebrider blade is able to handle. When used as a drill, however, the rotation settings are much slower for microdebriders than a conventional high-speed drill (15,000 RPM maximum vs. 80,000 to 100,000 RPM, respectively) and thus microdebriders are not as effective at removing thick bone expeditiously (Fig. 12.1). Microdebrider blades come in a variety of angles and offer rotating ports (Fig. 12.2). This allows improved access to some hard-to-reach areas of the sinonasal tract. One example is the lateral recesses of the maxillary and sphenoid sinuses, another is the frontal recess. One drawback of using a curved blade is that there are increased rates of obstruction of the inner cannula with debris compared to that with straight cannulas.5 A recent study performed by Boone et al9 compared a brand new prototype (4.3-mm Medtronic Quadcut blade; Medtronic) with their standard model (4.0-mm Medtronic Tricut blade; Medtronic) to evaluate the issue with clogging. They created a surgical model representing polyp disease (raw oysters) and AFS (minced beef cat food), and found decreased rates of clogging with the prototype in the AFS model. Neither model clogged from the debris in the nasal polyp model.9 Figure 12.1 Medtronic Straightshot M4 microdebrider and 4-mm × 15-cm anterior skull base burr with a 15-degree bend. Figure 12.2 Medtronic Straightshot microdebrider with a 30- degree, rotatable blade. Recent advances include the ability of navigation systems to track the tips of microdebrider blades. This is most easily accomplished using optical-based systems that can track any rigid instrument or any blade, but a few select blades can now also be tracked using electromagnetic-based platforms as well. Some companies make specialty microdebrider blades with a specific task in mind. For instance, the inferior turbinate blade is a small-diameter blade (2.0 and 2.9 mm sizes) used to perform submucous resection of the vascular erectile tissue of the turbinate while preserving the overlying mucosa. Some models have a beveled guard on the tip of the blade, which can be used to penetrate into the substance of the turbinate and raise the soft tissue away from the turbinate bone, eliminating the need for another instrument change during the procedure. By sparing the surface respiratory epithelium, less crusting and synechiae formation occur following operation than that when cautery or surface-damaging techniques are employed for turbinate reduction. The incidence of osteitis of the concha, an uncommon complication of turbinate surgery, is also lower when this technology is used.10 Microdebriders are routinely used by many otolaryngologists as they are thought to spare adjacent mucosa, provide improved precision over standard (nonpowered) instruments, remove tissue more quickly, and provide better visualization as blood is continuously cleared. Despite these anecdotal opinions, however, there are few evidence-based studies actually supporting these contentions.6–8,11 Sauer et al conducted a prospective, double-blinded, randomized control trial comparing maxillary antrostomy and ethmoidectomy performed using a microdebrider with those performed with standard instruments. Each patient had the procedure performed bilaterally with one side serving as the internal control. They noted an improvement in symptom and endoscopic scores at 3 weeks in the microdebrider group, but no other differences were noted.12 It should be mentioned that operating room times and blood loss were not reported in this study. The ability to simultaneously suction blood away from the surgical field is especially advantageous during ESS for nasal polyps that can bleed considerably during removal. Significant bleeding intraoperatively can increase the risk of complications. Despite the proliferation of microdebriders and their effectiveness at continuously clearing blood from the field, one significant drawback to current platforms is that they do not actually decrease bleeding in any way. The most recent innovation in microdebrider technology now permits the added ability to control bleeding while retaining the shaving and suctioning capabilities of this class of instrument. The PK Diego (Gyrus ACMI-ENT Division, Bartlett, Tennessee, United States) has the ability to provide hemostasis by delivering bipolar energy to the end of its blade. The blade is surrounded by layers of insulation that sandwich inner and outer electrodes (Fig. 12.3A). The instrument can be set to low (10 watts [W]), medium (20 W), or high (40 W) power. One drawback to the current model is that it has a fairly small zone of bipolar cautery, which is located at the distal aspect of the blade, perpendicular to the suction aperture. Figure 12.3 (A) PK Diego bipolar-equipped microdebrider with straight blade. (B) Intraoperative view of PK Diego (*) being used to resect an encephalocele (E) along the skull base (arrowhead). A controlled study of 80 patients undergoing surgery for chronic rhinosinusitis with polyps found that the use of the bipolar-equipped PK Diego was associated with significantly less blood loss and shorter operative times compared with surgery performed using a conventional microdebrider.13 The fact that the PK Diego functions using bipolar instead of monopolar energy is also noteworthy, as this limits the transmission of heat to adjacent intraorbital and intracranial structures. The application of this instrument is also well suited for submucous inferior turbinate reduction where bleeding from the turbinate interior as well as from the entry site can be readily controlled. It can also be beneficial in the endonasal removal of vascularized tissues (e.g., adenoids or tumors) and lesions involving the skull base (Fig. 12.3B). Future advances in this technology will likely focus on improving the ability to provide hemostasis during tissue removal, improved torque generation for enhanced drilling capacity, continued improvements in ergonomics, and improving suction flow to decrease clogging (especially in curved blades). Like any other instrument, microdebriders have certain limitations that must be recognized if these tools are to be used effectively and safely.4,5 Microdebriders are heavier than conventional instruments and are electrically powered. This means that the tactile feedback during surgery is markedly diminished with microdebriders. This, in addition to the powered nature of these instruments and their use in close proximity to critical structures, has raised concerns about the safety of microdebriders in ESS. Bhatti et al described two cases of ocular injury, one resulting in restrictive ophthalmoplegia and the other in transection of the medial rectus.14
Microdebrider
Basic Science and Current Technology

Image courtesy: Medtronic, Jacksonville, Florida, United States.

Image courtesy: Medtronic, Jacksonville, Florida, United States.
Instrument Advantages and Evidence
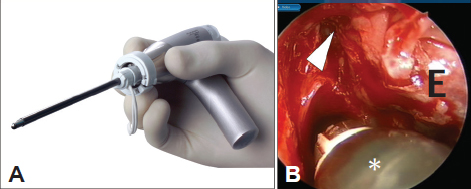
Images courtesy: Gyrus, Bartlett, Tennessee, United States.
Limitations
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


