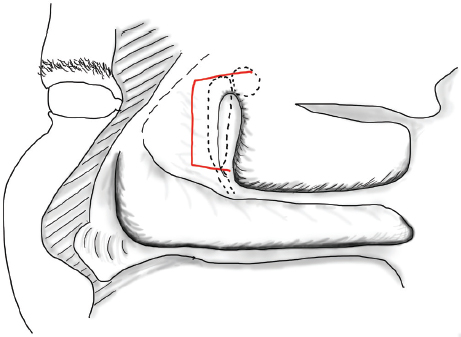
21 Powered Endoscopic Dacryocystorhinostomy The key concepts for successful, powered endoscopic dacryocystorhinostomy (DCR) are complete opening of the lacrimal sac, mucosa-to-mucosa apposition of the lacrimal sac mucosa to the nasal mucosa, and judicious stenting. This chapter begins with a description of the endonasal anatomy of the lacrimal sac before detailing the indications for powered endoscopic DCR, the procedure itself, the results, and complications. The endonasal anatomical relationships with the lacrimal sac are the axilla of the middle turbinate, the lacrimal bone, the frontal process of the maxilla, the uncinate process, and the agger nasi cell (Fig. 21.1). The axilla of the middle turbinate is the most prominent of these landmarks. It lies close to the opening of the common canaliculus into the lacrimal sac (at an average of 3 mm below the opening). Contrary to older anatomical descriptions, the upper border or fundus of the lacrimal sac projects an average of 8 mm above the axilla.1 Anterior and medial to the superior projection of the fundus of the sac lies the frontal process of the maxilla, which is composed of thick bone. This bone needs powered instruments to remove and achieve complete exposure of the lacrimal sac during endoscopic DCR. The axilla of the middle turbinate always attaches to the frontal process of the maxilla and not to the lacrimal bone. Thus, it becomes a medial relation of the upper part of the lacrimal sac as it projects anteriorly. The anterior border of the sac usually remains anterior to the attachment of the axilla.2 Removal of the axilla of the middle turbinate is, therefore, necessary during endonasal DCR. Figure 21.1 Diagram of the lateral wall of the nose showing positions of the lacrimal sac, agger nasi cell, maxillary line, and incisions for raising the initial mucosal flap. Below the axilla of the middle turbinate, the posterior half of the lacrimal sac is covered by the lacrimal bone and the anterior half by the frontal process of the maxilla. The lacrimomaxillary suture also corresponds to the point where the mucosa covering the medial aspect of the uncinate attaches to the lateral nasal wall. This can be visualized as a slight ridge running from the axilla of the middle turbinate to the upper border of the inferior turbinate called the maxillary line.3 The maxillary line is most exposed just above the upper border of the inferior turbinate so that during surgery, after elevation of a mucosal flap, the junction between the lacrimal bone and frontal process of the maxilla is most easily defined close to the inferior turbinate. Returning to the more complex anatomy of the lacrimal sac above the level of the axilla of the middle turbinate, the agger nasi cell (when present) will be related to the posterior lacrimal sac. In one study up to 55% of patients had anterior and medial pneumatization of this cell causing the agger nasi cell to overlap the posterior and posteromedial borders of the lacrimal sac.4 The agger nasi cell is therefore usually entered during complete exposure of the lacrimal sac. Even more medially, the upward projection of the uncinate process to its attachment on the middle turbinate, skull base, or medial border of the agger nasi can also overlap the posterior lacrimal sac above the axilla of the middle turbinate. The main indication is epiphora from nasolacrimal obstruction. Nasolacrimal obstruction is classified as either functional or anatomical. Functional obstruction occurs when investigations show no obvious obstruction of the system on dacryocystogram (DCG) investigation. However, lacrimal scintilography, which is a more functional investigation, will show no progression of the isotope from the eye to the nose. Anatomical obstruction is seen when the DCG shows obstruction of the system. If a patient presents with epiphora the eye should be examined for evidence of blepharitis or other causes of excessive tearing, and the eyelids should be checked for ectropion, entropion, and patency of the lacrimal puncta. Such abnormalities do not indicate DCR. If patent, the puncta can be cannulated and flushed with saline. Flow of saline through the other puncta indicates patency of the canaliculi, but if obstruction is at the level of the distal common canaliculus or beyond then powered endoscopic DCR is indicated. Reflux through the cannulated puncta indicates blockage of the canaliculus. Some clinicians rely on tactile feedback from probing to determine patency to the level of the lacrimal sac; a hard stop indicates abutment of the probe against the bone of the medial lacrimal sac wall and a soft stop indicates that the probe is stuck in the common canaliculus. Syringing, however, generates artificially high pressures in the nasolacrimal system that may overcome certain forms of obstruction and produce flow into the nasal cavity without reflux through the canaliculi. This is overcome by lacrimal scintilography where a radioactive dye is introduced into the conjunctival sac and later imaged to produce a lacrimal scintogram that may show failure of the dye to penetrate the lacrimal sac and/or nasal cavity. A combination of DCG and lacrimal scintography in the preoperative work-up for powered endoscopic DCR will determine the most likely area of narrowing and in particular, it will allow identification of common canalicular obstruction that may not be suitable for powered endoscopic DCR.5 Powered endoscopic DCR can also be used as a treatment for acute dacryocystitis.6 The endoscopic position of the lacrimal sac rarely varies and is mostly anterior to the orbit. Therefore, preoperative imaging of the nasal anatomy is not required. DCR begins with inspection of the nasal cavities to determine if a septoplasty is required. If, when using a 0-degree endoscope, the area of the axilla of the middle turbinate is not visible then septoplasty will facilitate surgical access and decrease the chance of postoperative adhesions. It is the senior author’s (P.J.W.) experience that a septoplasty is required in approximately 50% of cases. A limited endoscopic submucosal resection of the cartilage and bone in this area is usually sufficient.
Anatomy
Indications
Procedure
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


