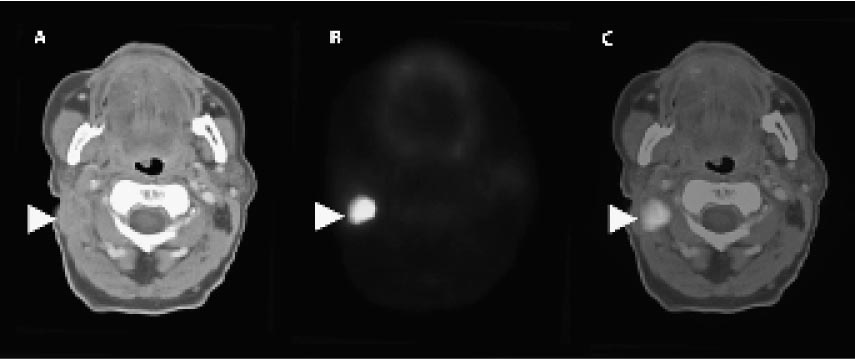
8 Positron Emission Tomography–Computed Tomography for the Head and Neck Over the last 10 years, several technological advances have improved the treatment of patients in the realm of head and neck cancer and endoscopic cranial base surgery. Combining computed tomography (CT) with positron emission tomography (PET) has improved the medical management and posttreatment surveillance of patients with squamous cell carcinoma (SCCa) and other malignancies of the head and neck. This technology has the promise of accurately detecting response to nonsurgical therapies and identifying persistent or recurrent disease that is not detectable by physical examination alone. Since the discovery that radioactive elements such as fluorine 18(18F) can be substituted in organic molecules, radioactive materials have been used in medical diagnosis and treatment. The fact that malignant tumors have increased glycolysis (the degradation of sugar for energy) allows the use of 2-fluoro-2-deoxy-D-glucose (18F-FDG) as a marker for tumor activity. Since the early 1990s, researchers have used 18F-FDG with PET for the identification of head and neck SCCa. Although excellent for identifying the presence of disease, PET does not allow a precise anatomical evaluation of the tumor site. In 2000, PET was combined with CT (PET-CT) images on a single acquisition platform to provide both tumor identification and anatomical detail Fig. 8.1). PET-CT has multiple applications for the identification, staging, and treatment of head and neck SCCa; however, there are several limitations. Fig. 8.1(A) Axial computed tomography (CT) image without contrast at the level of the mandible showing a large right level II lymph node (arrowhead). (B) Axial positron emission tomography (PET) image at the level of the mandible in the same patient showing 2-fluoro-2-deoxy-D-glucose (FDG) uptake in the right level II lymph node (arrowhead). (C) Axial combined PET-CT image at the level of the mandible in the same patient showing FDG uptake in the right neck consistent with a metastatic level II lymph node. Patients presenting with a head and neck SCCa require appropriate staging for treatment planning. Staging requires a detailed evaluation of the primary tumor site (T stage), the nodes (N stage), and metastatic sites (M stage), such as the lungs and liver. The combination of T, N, and M staging allows the physician to formulate a treatment plan and to educate the patient as to the success of treatment. A thorough history and physical examination, including imaging modalities, are required to stage SCCa. Multiple studies have shown that PET and PET-CT images have no advantage over traditional CT and magnetic resonance imaging (MRI) for evaluation of the primary tumor. The surgical oncologist gains little or no additional information about the primary tumor for surgical planning. However, a pretreatment PET allows the medical and radiation oncologist to follow tumor response to nonsurgical modalities (see discussion below). PET and PET-CT may have a role in identifying local or distant spread of SCCa prior to treatment. This knowledge may alter treatment planning by including or excluding either surgical or nonsurgical treatment regimens. Recent studies have shown a superiority of PET in identifying local (neck) and distant metastasis compared with CT and MRI. Indeed, PET has on average a 10 to 20% better chance of identifying tumor spread to the neck or lungs than traditional imaging modalities. Furthermore, PET has a very low false-negative rate (< 10%). Thus, the lack of 18
 Positron Emission Tomography
Positron Emission Tomography
 Evaluation and Treatment Planning
Evaluation and Treatment Planning
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


