Pigmented Tumors of the Cornea and Conjunctiva
Anh T. Q. Nguyen
Kathryn Colby
Pigmented lesions of the conjunctiva may be divided into melanocytic or nonmelanocytic lesions. Melanocytic lesions of the conjunctiva can be due to disorders either of melanocyte proliferation (melanocytosis) or of melanin production. The melanocytic lesions may be further subdivided into primary and secondary lesions, which may be congenital or acquired, and benign or malignant. In this chapter, the primary melanocytic lesions of the conjunctiva including conjunctival melanosis and its two subsets epithelial (racial) melanosis and subepithelial (congenital) melanocytosis are reviewed. Conjunctival nevi, primary acquired melanosis (PAM), and malignant melanoma are also discussed.
Melanocytes are cells of neural crest origin that migrate to mucus membranes, including the conjunctiva, and to the skin during embryogenesis (1). They reside in the basal layers of the conjunctival epithelium near the basement membrane. Conjunctival melanocytes closely resemble the dendritic melanocytes of the skin. Melanocytes contain melanosomes, which synthesize and store melanin and are therefore responsible for mucus membrane and skin pigmentation. Melanin may be released from melanocytes and taken up by epithelial cells. Skin and mucous membrane pigmentation in individuals with darker complexions is usually due to increased synthesis and release of melanin, rather than to an increase in the number of melanocytes. Conjunctival melanocytes are divided into three main types: dendritic cells that are located in the basal layer of the epithelium, intraepithelial nevus cells, and subepithelial fusiform melanocytes (2).
MELANOSIS
Epithelial Melanosis
Clinical Presentation
Epithelial or racial melanosis of the conjunctiva is a primary melanotic condition affecting blacks more commonly than whites (3,4). Racial melanosis first appears in early childhood and stabilizes in early adulthood. Typically, flat patches of pigment are scattered in the conjunctival epithelium, most commonly in the interpalpebral and perilimbal areas (Fig. 42-1). Both eyes are usually affected, although the amount of pigment may be asymmetric. The lesions commonly fade near the fornices. Because of their intraepithelial location, these pigmented lesions are freely mobile over the globe. The pigmentation may extend into the peripheral cornea and may be especially pronounced around the perforating branches of the anterior ciliary nerves.
Histopathology
Histopathologic examination of epithelial melanosis reveals an increased deposition of melanin granules in the basal layer of the conjunctival epithelium (3,4). The conjunctival epithelium shows normal morphology and maturation. The pigment does not extend further than the basal epithelium and there is no cellular atypia.
Treatment and Prognosis
Epithelial melanosis is a benign condition. Treatment consists of periodic observation. Care should be taken to distinguish racial melanosis from primary acquired melanosis, especially in darkly pigmented patients, where this distinction may be difficult (3). Biopsies maybe useful to confirm the histopathologic diagnosis if there is any concern.
Subepithelial Melanocytosis
Clinical Presentation
Subepithelial (congenital) melanocytosis of the deep conjunctiva, episclera or superficial sclera is a congenital condition that is more common in African Americans, Asians, and Hispanics (3,4). On examination, the pigmented lesions appear bluish or slate-gray and are usually unilateral (Fig. 42-2). Unlike epithelial melanosis, these lesions are deep and immobile. The overlying conjunctiva is not pigmented.
The melanocytosis may also affect the uvea, meninges, and soft tissues of the orbit. Ipsilateral dermal melanocytosis
in the distribution of the ophthalmic and maxillary branches of the trigeminal nerve may be found in approximately 50% of patients with congenital melanocytosis. This is referred to as oculodermal melanocytosis or nevus of Ota (4).
in the distribution of the ophthalmic and maxillary branches of the trigeminal nerve may be found in approximately 50% of patients with congenital melanocytosis. This is referred to as oculodermal melanocytosis or nevus of Ota (4).
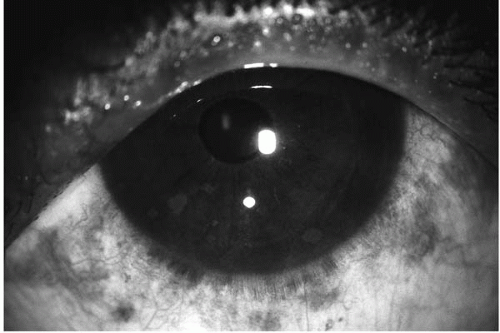 FIGURE 42-1. Racial melanosis in a 45-year-old black woman with neurofibromatosis. Lisch nodules are an incidental finding.(see color image) |
Histopathology
Treatment and Prognosis
The overall prognosis is good. However, white patients with the lesion have an increased risk of developing uveal melanoma (3,4). Glaucoma associated with hyperpigmentation of the trabecular meshwork develops in up to 10% of patients. Yearly ophthalmic evaluation is recommended.
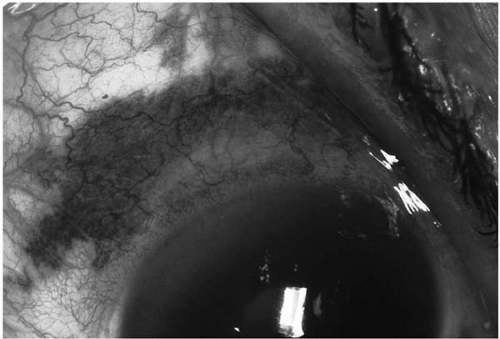 FIGURE 42-2. Ocular melanocytosis revealing deep flat, slate gray pigment. The overlying conjunctiva is not pigmented. (Photo courtesy of Frederick A. Jakobiec, M.D., with permission.) |
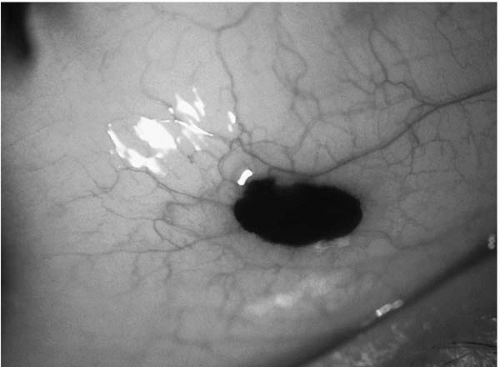 FIGURE 42-3. Small localized pigmented conjunctival nevus in a 12-year-old boy.(see color image) |
Conjunctival Nevi
Classification and Clinical Presentation
Nevi are common lesions of the conjunctiva. Their color ranges from tan to dark brown (Figs. 42-3 and 42-4). As many as 30%, however, may be lightly pigmented or even nonpigmented (Fig. 42-5). Pigmentation may increase during puberty, and previously nonpigmented lesions can become pigmented, making it seems as if the lesion has grown.
Nevi may be congenital, but more commonly arise during childhood or early adulthood. Similar to skin nevi, conjunctival nevi are classified by the layer in which they are found into intraepithelial (junctional), compound, or subepithelial nevi (2,4,5). It is difficult to distinguish the layer involved on clinical exam only. Nevi have little or no malignant potential.
Conjunctival nevi are usually solitary, well-circumscribed, flat to slightly elevated, brown, pigmented, freely mobile lesions most commonly found near the limbus (2,4,5).
Nevi may be focal or diffuse, but are almost never multifocal. Many nevi contain small cysts (Fig. 42-6).
Nevi may be focal or diffuse, but are almost never multifocal. Many nevi contain small cysts (Fig. 42-6).
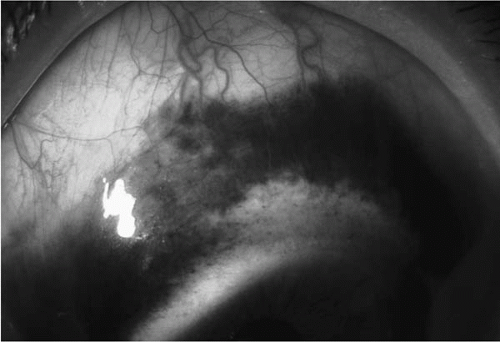 FIGURE 42-4. Diffuse pigmented conjunctival nevus in a 30-year-old Hispanic man. The lesion is brown rather than slate gray (cf. Fig. 42-2). The superficial location of the pigment is the conjunctiva is confirmed by the fact that the lesion is freely mobile with a surgical sponge. |
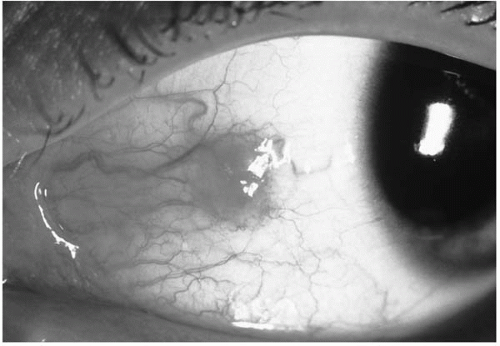 FIGURE 42-5. Nonpigmented conjunctival nevus. (Photo courtesy of Frederick A. Jakobiec, M.D.) |
Blue nevi differ from the more common nevi described above in that they are deeper, more localized, have a palpable thickness, and are more cellular (5,6). They are characteristically gray or blue in color and usually appear early in childhood. Blue nevi are usually benign, but have malignant potential if they are hypercellular (6,7).
Split nevus of the eyelid, a rare entity, has been reported in association with malignant melanoma of the conjunctiva (8).
Histopathology
Histopathologic examination of conjunctival nevi typically reveals spindle-shaped or multipolar dendritic cells full of fine melanin granules (nevus cells). The location of these cells determines if the nevus is junctional, subepithelial, or compound. In junctional nevi, nests of nevus cells are found at the junction between the epithelial and subepithelial tissues. Junctional nevi may occasionally be difficult to differentiate from PAM with atypia or melanomas due to histopathologic similarities. In contrast to PAM and melanomas, however, junctional nevi usually occur during childhood and pagetoid (intraepithelial) spread is rare.
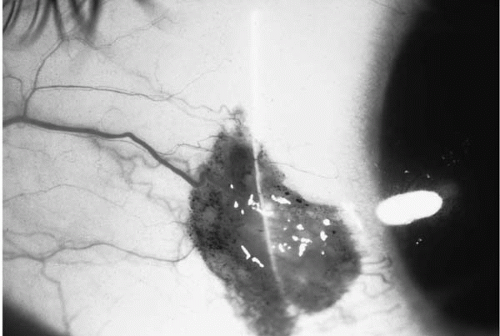 FIGURE 42-6. Conjunctival nevus illustrating characteristic clear cysts. (Photo courtesy of Frederick A. Jakobiec, M.D.)(see color image) |
Compound nevi of the conjunctiva show nevus cells both within and beneath the epithelium. In subepithelial nevi, the cells are located beneath the epithelium. Another variant, the combined nevus, is contains both a blue nevus and a junctional, compound, or subepithelial nevus (9,10). The blue nevus part of a combined nevi is usually smaller and deeper than the other component (9,10). Less common conjunctival nevus variants include the balloon cell nevus, the nevus of Spitz, and the pigmented spindle cell nevus of Reed (11).
Treatment and Prognosis
Nevi are benign lesions and most do not require treatment or surgical excision. Occasionally, nevi may become inflamed and may exhibit periods of rapid growth leading to the clinical suspicion of malignancy (12). The rapid growth typically occurs around puberty and is most commonly seen in compound nevi near the limbus. Patients with a history of allergies can also be prone to this phenomenon. Histopathology confirms the benign, inflammatory nature of these nevi.
Nevi of the palpebral conjunctiva, fornix, caruncle, and cornea are rare. Pigmented lesions in these locations, therefore, should be suspected of being malignant and an excisional biopsy performed.
Primary Acquired Melanosis
Clinical Presentation
PAM of the conjunctiva consists of unilateral, multiple, flat, indistinct areas of golden to dark brown coloration with irregular margins (1,2,4,13) (Fig. 42-7). The size and color of PAM lesions may change over time. The lesions are
usually freely mobile and may involve any part of the conjunctiva (1,5,13). Slit-lamp biomicroscopy, therefore, should include lid eversion with careful inspection of the palpebral conjunctiva (Fig. 42-8). Double eversion of the upper lid may be needed to inspect the entire upper fornix. The lacrimal gland and lacrimal sac are rarely involved by PAM (1,13).
usually freely mobile and may involve any part of the conjunctiva (1,5,13). Slit-lamp biomicroscopy, therefore, should include lid eversion with careful inspection of the palpebral conjunctiva (Fig. 42-8). Double eversion of the upper lid may be needed to inspect the entire upper fornix. The lacrimal gland and lacrimal sac are rarely involved by PAM (1,13).
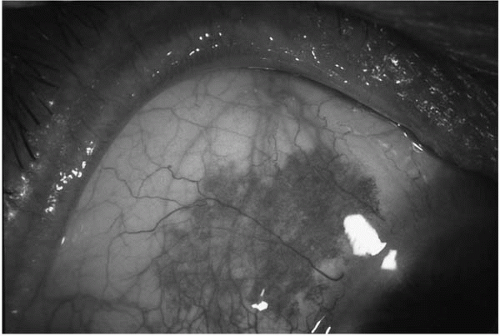 FIGURE 42-7. Primary acquired melanosis (PAM) in a 65-year-old Caucasian man showing characteristic golden brown color. The lesion is localized, flat, and freely mobile. |
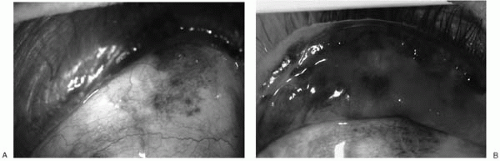 FIGURE 42-8. A: Diffuse PAM with atypia on the bulbar conjunctiva of a 75-year-old man. There is pigment at the mucocutaneous junction of the upper lid. B: Lid eversion demonstrates involvement of the upper palpebral conjunctiva. Examination of the entire conjunctiva is essential for appropriate management of patients with pigmented conjunctival tumors. |
PAM is relatively common in middle-aged or elderly whites and is extremely rare in blacks of all ages (1,13). The reported prevalence of PAM in the general population ranges from 10% to 36% (1). The melanosis in PAM is caused by an increase in melanin production with or without melanocytosis.
Malignant transformation of PAM lesions is common when histologic atypia is present (1, 2, 3, 4, 5,13,14). Overall, almost one half of patients with PAM with atypia will progress to melanoma. This rate approaches 90% for lesions that show epithelioid cells or a pagetoid growth pattern (13). Malignant transformation should be suspected in enlarging, highly vascularized lesions, lesions greater than 7.5 × 10 mm, or in lesions with patchy pigmentation (1,13). Development of one or more nodules in a previously flat lesion is an ominous sign.
Histopathology
Clinical features alone cannot distinguish precancerous PAM (with histologic atypia) from benign PAM without atypia (1,4). Suspicious lesions, therefore, should undergo an excisional biopsy, as this is the only way to determine the presence or absence of atypia.
Lesions without histologic atypia almost never become malignant (1,2,4,13). Histologically, PAM lesions without atypia may exhibit increased melanin production with or without melanocytosis (2). The melanocytosis in these lesions is usually restricted to the basilar regions of the conjunctival epithelium. Nuclear hyperchromasia is usually absent and the nucleoli are not prominent. Patients with PAM without atypia tend to be younger than patients with PAM with atypia (13). PAM without atypia may progress to PAM with atypia.
PAM with atypia has a significantly increased chance of malignant transformation. Five different patterns of atypical cells have been described with varied rates of progression to melanoma (1,13). These include small polyhedral cells, spindle cells, large dendritiform melanocytes, epithelioid cells, or polymorphous (mixture). The degree of atypia increases with the size of the nucleus and prominence of the nucleoli. These cells may remain in the basilar epithelial layer, form nests throughout the epithelium, spread to all levels of the epithelium in a pagetoid fashion, or proliferate in a sheetlike fashion. Lesions composed primarily of epithelioid cells or exhibiting pagetoid spread have the highest rate of malignant transformation (1,13).
Immunohistostaining with the monoclonal antibodies MIB-1 and PC-10 that stain for the proliferation markers Ki-67 and the proliferating cell nuclear antigen (PCNA) respectively, may help differentiate between PAM with and without atypia (15). It is still unclear, however, if staining with these proliferation markers is better at predicting the potential for malignant transformation than traditional histologic criteria (15, 16, 17, 18, 19, 20, 21).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


