This article reviews the various treatment methods for airway obstruction and feeding difficulty in infants with Pierre Robin Sequence (PRS), and highlights the benefits and limitations of early mandibular distraction osteogenesis in particular as a way of managing both airway obstruction and feeding difficulty in these children.
- •
Pierre Robin Sequence (PRS) is a triad of micrognathia, glossoptosis, and cleft palate, which may occur as isolated findings in an otherwise normal child or be associated with additional syndromic features.
- •
Children with PRS may exhibit varying degrees of upper airway obstruction.
- •
Management of upper airway obstruction is best approached conservatively, using nonoperative interventions first.
- •
The majority of infants are stabilized by nonsurgical measures.
- •
Children with neurologic deficits at risk for chronic aspiration are better served by traditional surgical interventions such as tracheotomy and gastrostomy-tube placement.
- •
Mandibular distraction osteogenesis is the only surgical technique that directly addresses the underlying cause of upper airway obstruction in PRS without compromising feeding. It offers results that persist through early childhood.
- •
Mandibular distraction procedure mandates specialized training.
- •
Complications of neonatal mandibular distraction osteogenesis:
| Short Term | Long Term |
|---|---|
| Infection | Tooth loss |
| Hardware failure | Scarring |
| Bone resorption and regression | Asymmetry |
| Nonunion | Corrective orthodontics |
| Facial nerve injury | Additional surgeries |
| Open-bite deformity |
PRS was first described in 1923 by Pierre Robin, a French stomatologist, as a diad of micrognathia and glossoptosis. In 1934 he revised the definition to include a triad of micrognathia, glossoptosis, and a U-shaped cleft palate. It is not a syndrome in itself, but rather a sequence in which multiple secondary anomalies are derived from a single anomaly, and affects approximately 1 in 8500 births. The prevailing hypothesis implicates hypoplasia of the mandible (either from a primary growth disturbance or from hyperflexion of the neck) before 9 weeks in utero as the inciting factor. The small jaw positions the tongue posteriorly and superiorly where it lies between the 2 palatal shelves, physically preventing their fusion, which normally occurs between the 8th and 10th weeks of gestation. It is this mechanical disruption of palatal closure and not a primary molecular or genetic factor that leads to the palatal cleft. Many newborns with PRS have upper airway obstruction and exhibit varying degrees of respiratory distress, which may require intervention. In addition, children may struggle with oral feeding, owing to the difficulty in coordinating breathing and swallowing in the context of tongue-base obstruction and a cleft palate.
Diagnosis of Pierre Robin Sequence
The diagnosis of PRS is typically made at birth. With improvements in prenatal imaging including high-resolution ultrasonography, micrognathia is now being diagnosed as early as the second trimester of pregnancy. In light of this there has been an attempt to standardize mandibular measurements on ultrasonography, including comparison with other cephalometric proportions and creation of a mandibular index, which takes into account the anterior/posterior dimension of the mandible as it relates to the biparietal diameter of the fetus. In practice, however, these measurements are rarely used, and micrognathia is often a relatively subjective call by the examining maternal fetal medicine physician. Inspection of the mandible is possible with ultrasonography, but evaluation of the tongue and palate is less reliable. Although the diagnosis of micrognathia can be made in utero, confirmation of the complete triad of PRS before delivery is usually not possible.
Physical Examination
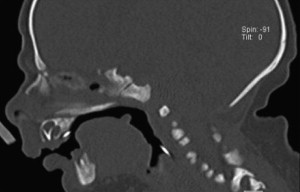
At birth, the micrognathia is the most striking feature. This trait is characterized by a small and retrusive mandible in which the mandibular alveolus is significantly posterior to the maxillary alveolus. Examination of the oral cavity reveals posterior and superior positioning of the tongue ( Fig. 1 ). Palatal examination will show a U-shaped cleft palate involving the soft palate and posterior hard palate; the alveolus is spared. Often the tongue is positioned within the palatal cleft itself, especially when the child is supine.
Some infants exhibit minimal respiratory symptoms at birth whereas others have significant airway obstruction, with stertor, retractions, and even cyanosis. These symptoms are usually worse when the child is lying supine, owing to gravity-dependent tongue-base obstruction, which occurs at the level of the oropharynx.
PRS may be the only abnormality noted on newborn examination, or may be noted as part of several dysmorphic features owing to a unifying, syndromic diagnosis. For this reason, some children with PRS are robust and vigorous, whereas others may have significant hypotonia (due to underlying neurologic impairment) or worrisome cyanosis (due to structural heart disease, for example). Examination of the ears, eyes, heart, and extremities may point toward a diagnosis of Nagar, Stickler, or velocardiofacial syndrome, to name a few. For this reason a full evaluation by a geneticist is helpful for categorizing infants with PRS into those with isolated findings and those with additional syndromic features. Children with neurologic impairment are at a higher risk than their peers with isolated PRS of requiring surgical intervention for airway distress.
Endoscopic Examination
Additional evaluation of the airway obstruction with fiberoptic nasal laryngoscopy is useful. Endoscopic examination usually confirms tongue-base obstruction and may identify synchronous airway lesions such as laryngomalacia. Additional causes of upper airway obstruction have been described in PRS, including lateral pharyngeal wall motion and pharyngeal narrowing without glossoptosis. While most children with PRS suffer from obstruction related to glossoptosis, indentifying these other variants is essential, as choosing the appropriate airway intervention requires accurate identification of the site of obstruction. For this reason not all children with PRS are effectively managed with interventions that target tongue-base obstruction alone.
Polysomnography
Quantifying the degree of respiratory compromise can be challenging. Polysomnography may be used to document the extent of airway obstruction and rule out any potential aspect of central apnea contributing to the infant’s respiratory distress. Often polysomnography is not necessary or even possible, for that matter, as many children have life-threatening airway obstruction when awake, obviating evaluation when they are unconscious.
Laboratory Studies
Laboratory studies may be used to support the diagnosis of chronic airway obstruction in those children without frank respiratory failure. Serial capillary blood gases may be used to document a trend of elevated or increasing carbon dioxide levels, thus suggesting chronic hypoventilation or worsening carbon dioxide retention.
All children with PRS should be observed in a monitored setting such as the neonatal intensive care unit, where continuous-pulse oximetry and cardiac monitoring are used.
Initial airway management for micrognathia
There is a variety of options available for airway management in the micrognathic child. Some children require no intervention whatsoever. However, many infants do display signs of upper airway obstruction, and when this occurs it is most reasonable to begin with the most conservative measures. The authors’ philosophy is to start with side and prone positioning. If the problem persists, placement of a nasopharyngeal airway can be helpful in both bypassing the tongue-base obstruction and in breaking the seal made between the oropharyngeal tongue and the posterior pharyngeal wall ( Fig. 2 ). A variety of custom oral appliances may also be fashioned for the purpose of relieving obstruction, and the literature is replete with reports on institutional experiences with these devices. Other investigators have described success at using customized endotracheal tubes to relieve obstruction.
Initial airway management for micrognathia
There is a variety of options available for airway management in the micrognathic child. Some children require no intervention whatsoever. However, many infants do display signs of upper airway obstruction, and when this occurs it is most reasonable to begin with the most conservative measures. The authors’ philosophy is to start with side and prone positioning. If the problem persists, placement of a nasopharyngeal airway can be helpful in both bypassing the tongue-base obstruction and in breaking the seal made between the oropharyngeal tongue and the posterior pharyngeal wall ( Fig. 2 ). A variety of custom oral appliances may also be fashioned for the purpose of relieving obstruction, and the literature is replete with reports on institutional experiences with these devices. Other investigators have described success at using customized endotracheal tubes to relieve obstruction.
Surgical interventions for upper airway obstruction
Nonsurgical management of upper airway obstruction in children with PRS is not only possible; it is preferable. Retrospective reviews examining airway interventions in infants with PRS consistently demonstrate that most children may be successfully managed nonoperatively. Nevertheless, some patients are unable to tolerate oropharyngeal stents or nasopharyngeal airways; management of these devices may prove overwhelming to providers and parents alike.
Surgical interventions to address tongue-base obstruction in PRS
Tongue-Lip Adhesion
A variety of glossopexy procedures have been described including tongue-lip adhesion (TLA), which may be performed with or without subperiosteal release of the floor of mouth and circum-mandibular suturing. In one popular technique, the genioglossus musculature is released from the mandible and the circum-mandibular suture technique is used to anchor the tongue-base to the inferior alveolus. Mucosal flaps, which were raised from the ventral tongue and the ends of the gingivolabial sulcus are then brought together to complete the adhesion ( Fig. 3 ). The adhesion is maintained throughout the first year of life and is typically taken down at the time of palate repair, which takes place at approximately age 9 to 12 months. Although the success rate of this technique at managing airway obstruction is as high as 89% in select patients, tethering the mobile tongue anteriorly tends to exacerbate the child’s underlying dysphagia, increasing the likelihood of requiring a prolonged period of enteral feeding supplementation via nasogastric catheter or gastrostomy tube. In a recent review of a single institution’s experience with TLA, 54% of children in whom airway obstruction was successfully managed by this procedure required gastrostomy-tube placement to assure adequate nutritional intake. In 1998, a survey of airway surgeons at pediatric centers caring for children with PRS suggested that more than 80% of institutions have abandoned this technique. However. the minority of centers who still use TLA believe it is a worthwhile intervention and are satisfied with their results. Advocates cite the relative simplicity of the procedure, lack of long-term scarring, avoidance of potential nerve or tooth injury, and lack of specialized equipment as major advantages of the TLA technique over more complex and expensive orthognathic procedures. Critics of the technique cite variable results and significant postoperative dysphagia requiring prolonged nasogastric or gastrostomy-tube feeding. For this reason the authors believe that those children who can be stabilized with TLA are likely the same group of patients successfully managed with nasopharyngeal airways with or without nasogastric feeding.
Tracheotomy
Traditional algorithms for airway management in children with PRS point to the use of tracheotomy as a final backup for children who fail TLA, as it is considered the definitive technique for securing a stable airway in any patient with upper airway obstruction. Although a tracheotomy will reliably and successfully bypass the site of tongue-base obstruction, it is a procedure with potential long-term morbidity and mortality. Complications associated with tracheotomy include:
- •
Sudden airway obstruction from accidental decannulation or mucous plugging
- •
Airway infections
- •
Bleeding
- •
Stomal maintenance problems
- •
Tracheal stenosis
- •
Inhibition of proper speech and swallowing development.
Furthermore, children with tracheotomies require skilled nursing care at home and in their educational facilities, along with monitoring and suction equipment, among other resources. Nevertheless, in a survey of otolaryngologists at large fellowship training centers, 52% chose tracheotomy as the treatment of choice for airway management in children with PRS.
Mandibular Distraction Osteogenesis
Another option for the management of airway obstruction in the neonatal period is mandibular distraction osteogenesis (MDO). This technique, in which the mandible is slowly advanced after an initial osteotomy, relieves supraglottic airway obstruction by bringing the tongue base forward ( Fig. 4 ). This surgery is now widely used across the United States for select children with micrognathia and severe airway obstruction as an alternative to tracheotomy. This technique is gaining wider acceptance among plastic craniofacial surgeons and pediatric otolaryngologists alike, as feeding outcomes in general are more favorable than those observed with TLA, allowing children to avoid both a tracheotomy and a gastrostomy tube in most cases. The specifics of patient selection, operative technique, and protocol for postoperative distraction are described later in this article. Potential early and long-term complications are also discussed.



