Physical Injuries of the Cornea
Puwat Charukamnoetkanok
Mahnaz Nouri
Roberto Pineda Ii
Physical injury to the cornea can have potentially devastating consequences to the vision and health of the eye. However, a poorly prepared plan to repair the injury without careful evaluation and initiation of appropriate treatments can lead to a suboptimal outcome that is equally visually unsatisfying. This chapter discusses important considerations in the evaluation of corneal blunt trauma and perforating injuries, highlights appropriate treatment recommendations directed by theoretical or evidence-based support, and discusses other physical injuries of the cornea including thermal injuries, phacoemulsification-related corneal trauma, and traumatic injuries related to corneal refractive surgery.
BLUNT TRAUMA OF THE ANTERIOR SEGMENT
Blunt Corneal Trauma
Severe intraocular damage to the eye can occur even when the force of injury is insufficient to rupture the globe (open-globe injury). Fortunately, the effects of blunt trauma on the healthy cornea are usually transient (1). For example, a direct, focal, concussive force from BB pellet or paint ball results in mechanical injury to the surrounding endothelium manifesting as a ring of corneal edema (2).
Blunt trauma with severe corneal contusion may result in a rupture of Descemet’s membrane. The resultant breach of the endothelial barrier leads to acute hydrops, characterized by marked corneal edema similar to that seen with keratoconic hydrops. However, healthy endothelium is capable of healing such ruptures by sliding or migrating over the area of retracted Descemet’s membrane. This mechanism restores the normal endothelial pump and barrier functions necessary to maintain corneal deturgescence, and usually occurs over 3 months. Routinely, on clinical slit-lamp examination, a footprint of parallel striae or a fishmouth break in Descemet’s membrane can be found. These lesions are visual indicators of previous traumatic events but seldom result in significant visual impairment of vision. Numerous treatment modalities have been proposed including patching, bandage soft contact lens, topical corticosteroids, topical glaucoma medications, hypertonic sodium chloride preparations, anterior chamber air or expansible gases, as well as thermokeratoplasty, however their usefulness remains unproven (1).
Corneal rupture is uncommon following blunt trauma unless the eye has predisposing risk factors including corneal ectatic pathology such as keratoconus, pellucid marginal degeneration, Terrien’s marginal degeneration, or prior corneal surgery such as penetrating keratoplasty (3), or incision surgery such as radial or astigmatic keratotomy.
Corneal Abrasions
Corneal abrasions, partial or complete removal of the corneal epithelium, are one of the most common ocular injuries. Studies have estimated that corneal abrasions account for 10% of new patient visits to the eye emergency room (4) and occur in 3.5% of the population (5). Tangential impact from foreign bodies, including fingernails, paper, plants, or brushes, is the most frequent cause of corneal abrasions. It is also frequently encountered in ocular chemical or thermal injuries.
The basal cells of the corneal epithelium rest on a basement membrane and are anchored to the stroma by hemidesmosomes (6). Corneal scarring does not occur with traumatic epithelial abrasions. However, if the abrasion extends beyond the epithelial basement membrane and the underlying Bowman’s layer and corneal stroma are violated, corneal keratocytes are activated, resulting in new collagen deposition and cicatrix formation. Scarring will occur if Bowman’s layer is violated or the underlying corneal stroma is involved in the trauma.
Clinically, patients often present with symptoms of pain, photophobia, foreign-body sensation, and tearing. An irregular or denuded ocular surface may result in decreased vision that may not improve with pinhole visual acuity testing. The presence of an abrasion can be confirmed by application of fluorescein dye, which highlights the epithelial defect in apple green when viewed with a cobalt blue light.
Examination of a corneal abrasion should focus on the extent of abrasion, the degree of stromal involvement, and the presence of other associated injuries. As in all eye trauma, the examiner must be mindful of the possibility of occult ocular injuries such as an open globe or retained intraocular foreign body. A corneal abrasion may be the only clue of a high-velocity foreign object that may pass completely through the cornea with minimal disturbance of the corneal anatomy (7,8).
Most corneal abrasions resolve without long-term complications within 24 to 72 hours (9). Therefore, the aims of therapy are to maximize the patient comfort, promote epithelial healing, and prevent complications. Common treatment modalities include topical antibiotics, cycloplegic agents, and ocular patching or a bandage soft contact lens.
The corneal epithelium provides a principal barrier against harmful organisms, and because the mechanism of injury is usually a dirty foreign body, a major concern regarding corneal abrasion is the risk of microbial keratitis. Patients should be considered at high risk for corneal infection until re-epithelialization is complete. Instillation of broad-spectrum antibiotics is recommended for microbial prophylaxis. There is no study to date that demonstrates that any one antibiotic is better than another. However, it is important to note that almost all topical medications retard epithelial healing to some degree due to the presence of preservatives in the solution (10).
To alleviate patients’ pain, cycloplegic agents should be used to minimize ciliary spasm. Physicians should select agents with appropriate duration of action according to the extent of the injuries. A randomized, double-masked, placebo-controlled study demonstrated that when used as adjunctive therapy, ketorolac tromethamine 0.5% ophthalmic solution provided increased patients’ comfort without adverse effects (11).
Due to the risk of promoting infection, patching is clearly not recommended when corneal abrasion involves vegetable matter, wood, contact lens use, or other “dirty” materials. The efficacy of patching in relieving pain or promoting reepithelialization is controversial. A randomized clinical trial suggests that eye patching in children (aged 3 to 17 years) with isolated corneal abrasions makes no difference in the rate of healing (9). Gregersen et al. (12) reported faster epithelial healing and less subjective symptoms in patients with double eye patches for 24 hours than those patched for 6 hours. However, numerous studies have contradicted this finding, and have questioned the effectiveness of patching in support of no patching (13, 14, 15, 16).
Kaiser (14) conducted a large-scale, randomized, controlled trial in patients with noninfected, non-contact lens-related traumatic corneal abrasions. The patients were treated with topical antibiotics and mydriatics and were randomized to receive either a pressure patch or no patch (14). The authors concluded that for small abrasion (<10 mm2), patients treated with antibiotic ointment and mydriatics alone had significantly faster healing times and lower pain level scores. The authors noted that pressure patching was not a benign treatment because it removed binocular vision and could be uncomfortable for the patient.
However, for large traumatic abrasions (>10 mm2), the study by Kaiser (14) found that the patched group had a faster healing time. The abrasion took 3.45 days to heal in the patch group, compared with 4.20 days in the nonpatch group. Due to the small number of patients with large abrasions, this study was not powered to detect a statistically significant difference. Nonetheless, the author recommends that, unless contraindicated, abrasions larger than 10 mm2 should continue to be patched until the effectiveness of pressure patching is established in this subset of patients by additional studies.
Alternatively, bandage soft contact lenses have been thought to be an attractive alternative to patching. It protects the epithelium from eyelids friction and promotes healing and reduces patient discomfort (17). Treating physicians must be careful of complications from contact lens such as an increased risk of infection and reduced oxygen permeability. Therefore, these patients may require closer attention for this form of therapy.
Corneal Foreign Body
Corneal foreign bodies are one of the most frequently encountered urgencies seen in ophthalmic practice. Patients with corneal foreign bodies are usually motivated to seek prompt medical attention because of ocular discomfort. Many particles may cause injury including glass, plastic, insect parts, plant debris, wood splinters, paint chips, and cinders (8). However, metal objects represent the most hazardous material to the eye.
Patients often present with pain, photophobia, excessive tearing, redness, and blurred vision. Particles that are hot and projected at high speed may become embedded in the stroma and not initially produce ocular discomfort. Patients often seek care when the eye becomes inflamed hours later and may not recognize that the foreign body is the cause of their symptoms. A detailed history is important for high-quality patient care and for medicolegal reasons. Transparent materials such as fiberglass and glass, which may be difficult to locate, can be more readily identified when the physician anticipates their presence. Furthermore, high-speed projectile objects may penetrate the eye with minimal evidence of entry (7). Careful slit-lamp examination is essential to observe location, depth, and type of particles. The globe should be assessed for signs of perforation such as hypotony, shallow anterior chamber, altered pupil size,
and a positive Seidel’s test. The upper and lower lid should always be everted to ensure that all debris has been removed. Treating physicians must be sure to ask about the patient’s tetanus status if metallic material is suspected and a tetanus booster administered if indicated.
and a positive Seidel’s test. The upper and lower lid should always be everted to ensure that all debris has been removed. Treating physicians must be sure to ask about the patient’s tetanus status if metallic material is suspected and a tetanus booster administered if indicated.
Metallic corneal foreign bodies must be removed. Particles lodged near the visual axis should be removed with care to minimize further injury to the cornea. Foreign bodies located at the level of Bowman’s layer or in the stroma will produce scarring regardless of the physician’s skill. However, not all foreign bodies require removal. Small inert materials such as glass may be left in the cornea.
Irrigation may be attempted to dislodge superficial foreign bodies by using sterile irrigating solution pointed at a slight angle to avoid further embedding the particle more posteriorly into the cornea. If irrigation is not successful, mechanical instrumentation should be used to dislodge the foreign body at the slit lamp. A stainless steel spud, shaped like a golf club or hockey stick, is very effective. Alternatively, the beveled tip of a sterile disposable small gauge needle can also be utilized. To prevent inadvertent penetration, the instrument should be held tangential to the cornea rather than perpendicular to it. Epithelial damage, either during the initial trauma or after removal of foreign body, is unavoidable. Patients should receive treatment for the corneal abrasion as well as the foreign body.
Iron-containing foreign bodies often produced rust rings that delay healing and may be a continuous source of irritation (22). Within hours of the corneal injury, rust stains adjacent epithelial cells and Bowman’s membrane, eventually diffusing into the corneal stroma.
Various instruments, including battery-powered drills (e.g., Alger brush) or needle tip, may be used to remove the rust ring (Fig. 44-1). These instruments are equally effective, although using a needle is generally more time-consuming (23). Extraction of the rust ring may be difficult in a fresh corneal injury. The clinician may have to wait a few days and repeat the procedure when the surrounding tissue becomes softened and the rust has solidified. Every trace of the rust ring need not be removed because the retained particles will eventually extrude over time.
 FIGURE 44-1. Battery-powered drills (Alger brush II) used to remove the rust ring from metallic foreign bodies. |
When multiple foreign bodies exist, removal of particles individually may result in excessive scarring. The debridement of the corneal epithelium may be a more appropriate approach to remove foreign bodies without excessively disrupting the integrity of Bowman’s layer (24).
Removal of deep corneal foreign bodies may be impossible if the size, contrast, or location precludes visualization by slit-lamp or surgical biomicroscopy. Au et al. (25) described a lamellar pocket technique for removal of a deep intrastromal corneal foreign body. In this technique, the foreign body was removed through a peripheral corneal incision minimizing unwanted distortion of the corneal topography. Yang (26) described a simple technique using the suture needle for removal of corneal foreign bodies that project into the anterior chamber. A 6-mm needle (10-0, micropoint spatula, Ethicon, United Kingdom) was used to pass just beneath the corneal foreign bodies, slightly lifting the cornea, and everting the anterior opening of the wound. The use of a suture needle enhanced visualization by providing reflection of light from the back, maintaining the anterior chamber, exposing the corneal foreign bodies, and stabilizing the globe. After removing the foreign body, the suture could then be tied as a temporary suture before placement of permanent suture(s).
Organic foreign bodies, such as those from plants and insects, pose an additional challenge due to increased risk of infection and inflammation (27). Patients should be followed closely, and if an infection does develop, the treating physician must maintain a high suspicion for the possibility of a
mycotic organism. Exposure to tarantula spiders demonstrates how insect parts can result in a significant inflammatory reaction of the cornea (28, 29, 30) (Fig. 44-2). Cooke et al. (31) classified tarantulas’ hairs into four types. Of these, type III (long, thin, with sharp points and multiple barbs) can embed and penetrate skin or cornea. Typical ocular responses to insect foreign bodies, termed ophthalmic nodosa, include conjunctival granulomas, corneal stromal infiltrate, and anterior chamber reaction (32). The goals of therapy are removal of the tarantula hairs and control of ocular inflammation. Long-term suppression of inflammation may be necessary until the hairs are resorbed (33).
mycotic organism. Exposure to tarantula spiders demonstrates how insect parts can result in a significant inflammatory reaction of the cornea (28, 29, 30) (Fig. 44-2). Cooke et al. (31) classified tarantulas’ hairs into four types. Of these, type III (long, thin, with sharp points and multiple barbs) can embed and penetrate skin or cornea. Typical ocular responses to insect foreign bodies, termed ophthalmic nodosa, include conjunctival granulomas, corneal stromal infiltrate, and anterior chamber reaction (32). The goals of therapy are removal of the tarantula hairs and control of ocular inflammation. Long-term suppression of inflammation may be necessary until the hairs are resorbed (33).
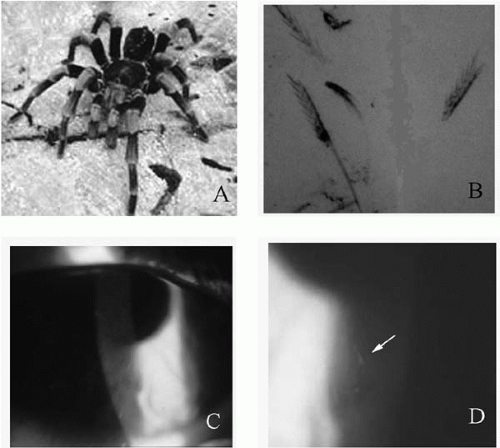 FIGURE 44-2. Tarantula keratits. A: Tarantula spider. B: High magnification examination of the tarantula hairs. C: Corneal edema. D: Higher magnification of the cornea demonstrating embedded tarantula’s hair (arrow).(see color image) |
Laser in situ keratomileusis (LASIK) has been associated with decreased corneal sensation. The increasing number of patients having LASIK suggests that corneal foreign bodies may become more common in this population. Porges et al. (34) reported nine eyes of eight patients who presented with corneal foreign bodies after LASIK. The removal was carried out with a 27-gauge needle with no flap-related complications. The authors recommended avoidance of antibiotic ointment to prevent a possible penetration of oily material beneath the flap. Interestingly, half of the patients did not realize that they had the corneal foreign bodies. Transient post-LASIK corneal hypoesthesia might explain this phenomenon. Protective eyewear should be an integral part of postoperative precaution in patients who have undergone refractive surgery.
After removal of corneal foreign bodies, the cornea will usually heal quickly without sequelae. However, if the basement membrane has been damaged, it may take up to 6 weeks or more to restore secure cellular attachments of the epithelium to the underlying basement membrane. Rarely, recurrent corneal erosions may complicate the posttraumatic injury and may occur weeks, months, or even years after the event (35).
Airbag Injuries
Because of mandatory installation of automotive airbags on all 1998 and later vehicle models, airbags have undoubtedly reduced the incidence of fatal and severe injuries in automobile collisions (36). However, numerous case reports of airbag-related eye injuries have been published (36, 37, 38, 39). Airbags are rubber-lined nylon bags folded into the steering column and dashboard. Upon deployment, combustion of sodium azide-generated nitrogen gas fills the 50-L volume of the airbags in 0.05 seconds, and propels it toward the automobile occupant at speeds of 100 to 200 mph (40). In addition, airbag deployment also generates heat, alkaline aerosols, and carbon dioxide.
Injuries related to automotive airbags constitute two major categories: mechanical injuries and chemical burns. The types of corneal injuries described with airbags include corneal abrasion, contusion, edema, corneal blood staining, and corneal laceration (41, 42, 43, 44, 45) (Fig. 44-3). At least one case of permanent bullous keratopathy after airbag trauma has been documented (46). In another case report, alkali burn of the eye was associated with airbag deployment (47).
Duma et al. (48) investigated 22,236 individual crashes in the United States from the National Automotive Sampling System database from January 1993 through December 1999. The authors proposed a new four-level eye injury severity
scale that quantifies injuries based on recovery time, need for surgery, and possible loss of sight. Three percent of automotive occupants who encountered airbag deployment sustained an eye injury compared with 2% of those who did not. This difference, however, was not found to be statistically significant. A closer examination of the type of eye injuries demonstrated a statistically significant increased risk of corneal abrasions for occupants exposed to airbag deployment. However, occupants from car crashes without airbag deployment sustained a greater number of severe ocular injuries. Characteristics of occupants and crashes, such as eyeglasses, contact lens, or seat belt uses, age, height, and crash velocity, were not significantly correlated with the risk of airbag-induced eye injury.
scale that quantifies injuries based on recovery time, need for surgery, and possible loss of sight. Three percent of automotive occupants who encountered airbag deployment sustained an eye injury compared with 2% of those who did not. This difference, however, was not found to be statistically significant. A closer examination of the type of eye injuries demonstrated a statistically significant increased risk of corneal abrasions for occupants exposed to airbag deployment. However, occupants from car crashes without airbag deployment sustained a greater number of severe ocular injuries. Characteristics of occupants and crashes, such as eyeglasses, contact lens, or seat belt uses, age, height, and crash velocity, were not significantly correlated with the risk of airbag-induced eye injury.
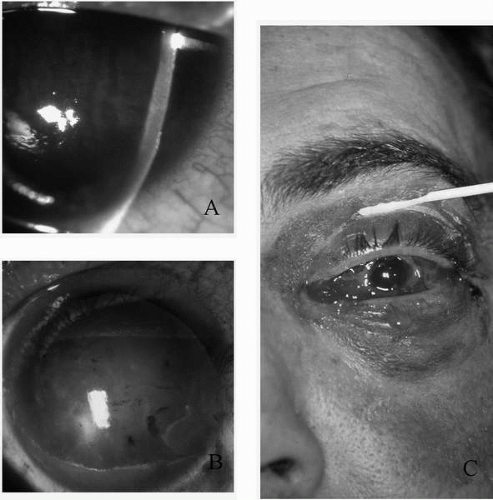 FIGURE 44-3. Consequences of airbag injuries. A: Corneal edema, which may result from chemical irritation or from the contusion injury. B: The impact can be severe enough to cause subluxation of crystalline lens. C: Blunt globe rupture presents with conjunctival injection and chemosis. |
Lehto et al. (49) performed a retrospective observational case series (n = 378) from data collected between 1993 and 1997 in Finland to evaluate the risk of eye injuries from airbag deployment and the relationship between eye injuries and eyewear. The authors reported a risk of 2.5% for any airbag-related eye injury and 0.4% for severe eye injuries. There was no significant difference in the risk for eye injury between survivors in accidents involving airbag deployment and those not involving airbags. Furthermore, eyeglasses or contact lens did not contribute to a greater risk of eye injuries. However, the power of this study was low because of the small number of individuals with ocular injuries.
The rising proportion of airbag-equipped cars as well as the increasing percentage of the population electing for corrective vision surgery are two converging trends that may increase the risk and severity of airbag-induced ocular injuries. Thus, innovation of airbag and eyewear protection designs is particularly needed. One such innovation is the development of airbags that would inflate at different speeds depending on the severity of the collision and the physical characteristics of the occupants.
PERFORATING INJURIES OF THE ANTERIOR SEGMENT
Corneal and Corneoscleral Lacerations
This section reviews important concepts related to corneal lacerations, including partial-thickness lacerations, simple full-thickness lacerations, angular and intersectional lacerations, and stellate lacerations. It also explores various issues pertaining to complicated anterior segment traumas, including corneoscleral lacerations with uveal prolapse or iris incarceration, corneoscleral laceration repair, and cataract extraction, as well as anterior segment intraocular foreign bodies. The fundamentally important mission of corneal laceration repair is complete watertight wound closure with restoration of corneal sphericity. Moreover, goals of wound repair should always include release of uveal and vitreous incarceration, prevention and management of infections, and preparation for secondary anterior segment reconstruction.
Keratorefractive Principles
Understanding of the micromechanical effects of penetrating injury and its repair is crucial for facilitating primary corneal restoration and maximizing ultimate visual outcome by managing astigmatism and corneal scarring (50). The corneal laceration itself along with its subsequent surgical repair as well as the tissue wound healing responses exert significant influence on residual astigmatism after the recovery.
Effect of the Laceration
Corneal incisions produce keratometric flattening over the affected region of the cornea due to wound gaping (51,52). Circumferential incisions (transverse or arcuate incisions) flatten the cornea along the meridian parallel to the incision while steepening the axis 90 degrees away. On the other hand, radial incisions flatten the cornea along both the axis of incision and the axis 90 degrees away (53).
The anatomy of the lacerations [vertical (perpendicular) or oblique (shelved or beveled)] affects gaping of the incision differently (Fig. 44-4). The valve rule of Eisner (54) states, “Incisions through the wall of the globe produce valves whose margin of watertightness is equal to the projection of the surface of the incision onto the surface of the globe.” Thus, vertical corneal lacerations gape more than shelved corneal lacerations. Moreover, incisions perpendicular to the cornea open spontaneously and require sutures for coaptation. By contrast, shelved incisions tend to close spontaneously.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


